

Severe Acute Respiratory Syndrome Coronavirus 2 Infections Among Children in the Biospecimens from Respiratory Virus-Exposed Kids (BRAVE Kids) Study
- PMID: 33141180
- PMCID: PMC7665428
- DOI: 10.1093/cid/ciaa1693
Severe Acute Respiratory Syndrome Coronavirus 2 Infections Among Children in the Biospecimens from Respiratory Virus-Exposed Kids (BRAVE Kids) Study
Abstract
Background: Child with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection typically have mild symptoms that do not require medical attention, leaving a gap in our understanding of the spectrum of SARS-CoV-2-related illnesses that the viruses causes in children.
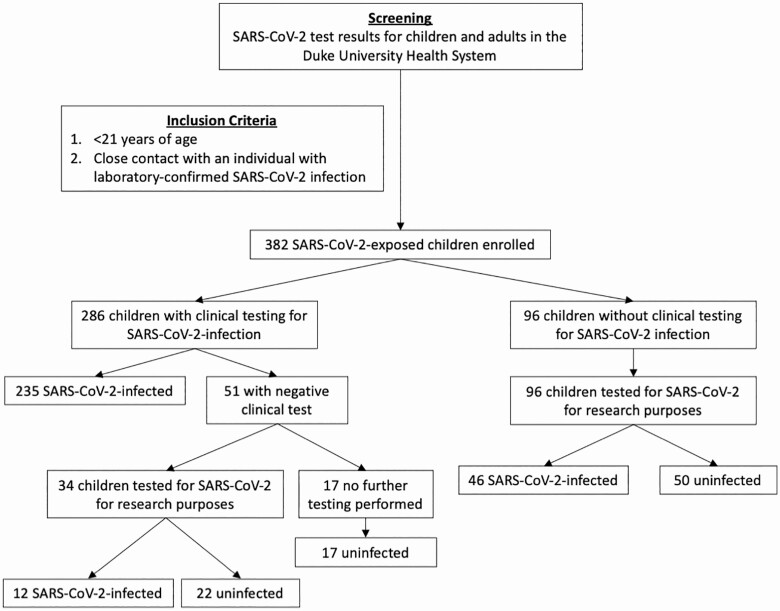
Methods: We conducted a prospective cohort study of children and adolescents (aged <21 years) with a SARS-CoV-2-infected close contact. We collected nasopharyngeal or nasal swabs at enrollment and tested for SARS-CoV-2 using a real-time polymerase chain reaction assay.
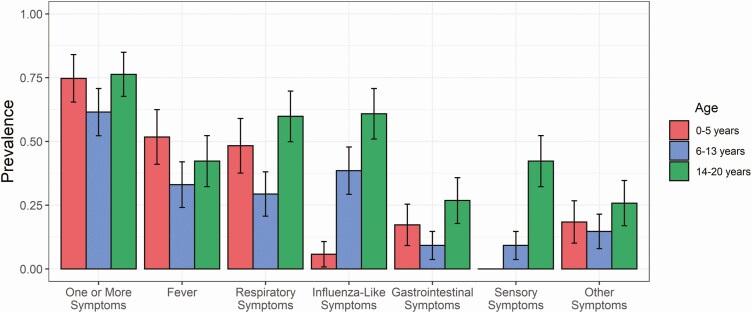
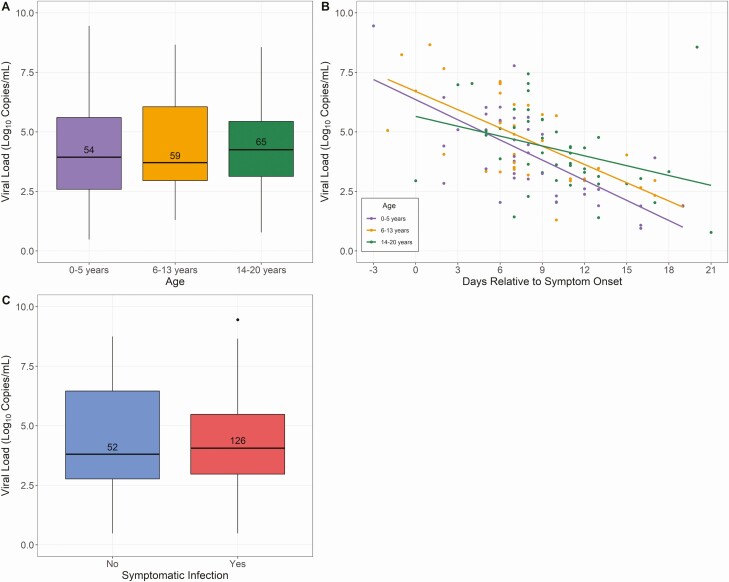
Results: Of 382 children, 293 (77%) were SARS-CoV-2-infected. SARS-CoV-2-infected children were more likely to be Hispanic (P < .0001), less likely to have asthma (P = .005), and more likely to have an infected sibling contact (P = .001) than uninfected children. Children aged 6-13 years were frequently asymptomatic (39%) and had respiratory symptoms less often than younger children (29% vs 48%; P = .01) or adolescents (29% vs 60%; P < .001). Compared with children aged 6-13 years, adolescents more frequently reported influenza-like (61% vs 39%; P < .001) , and gastrointestinal (27% vs 9%; P = .002), and sensory symptoms (42% vs 9%; P < .0001) and had more prolonged illnesses (median [interquartile range] duration: 7 [4-12] vs 4 [3-8] days; P = 0.01). Despite the age-related variability in symptoms, wWe found no difference in nasopharyngeal viral load by age or between symptomatic and asymptomatic children.
Conclusions: Hispanic ethnicity and an infected sibling close contact are associated with increased SARS-CoV-2 infection risk among children, while asthma is associated with decreased risk. Age-related differences in clinical manifestations of SARS-CoV-2 infection must be considered when evaluating children for coronavirus disease 2019 and in developing screening strategies for schools and childcare settings.
Keywords: COVID-19; asymptomatic; community; pediatric; viral load.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Update of
-
SARS-CoV-2 Infections Among Children in the Biospecimens from Respiratory Virus-Exposed Kids (BRAVE Kids) Study.medRxiv [Preprint]. 2020 Sep 1:2020.08.18.20166835. doi: 10.1101/2020.08.18.20166835. medRxiv. 2020. Update in: Clin Infect Dis. 2021 Nov 2;73(9):e2875-e2882. doi: 10.1093/cid/ciaa1693. PMID: 32908992 Free PMC article. Updated. Preprint.
References
-
- Davies NG, Klepac P, Liu Y, Prem K, Jit M, Eggo RM; CMMID COVID-19 Working Group . Age-dependent effects in the transmission and control of COVID-19 epidemics. Nat Med 2020; 26:1205–11. - PubMed
