

Association Between African American Race and Clinical Outcomes in Men Treated for Low-Risk Prostate Cancer With Active Surveillance
- PMID: 33141207
- PMCID: PMC7610194
- DOI: 10.1001/jama.2020.17020
Association Between African American Race and Clinical Outcomes in Men Treated for Low-Risk Prostate Cancer With Active Surveillance
Abstract
Importance: There is concern that African American men with low-risk prostate cancer may harbor more aggressive disease than non-Hispanic White men. Therefore, it is unclear whether active surveillance is a safe option for African American men.
Objective: To compare clinical outcomes of African American and non-Hispanic White men with low-risk prostate cancer managed with active surveillance.
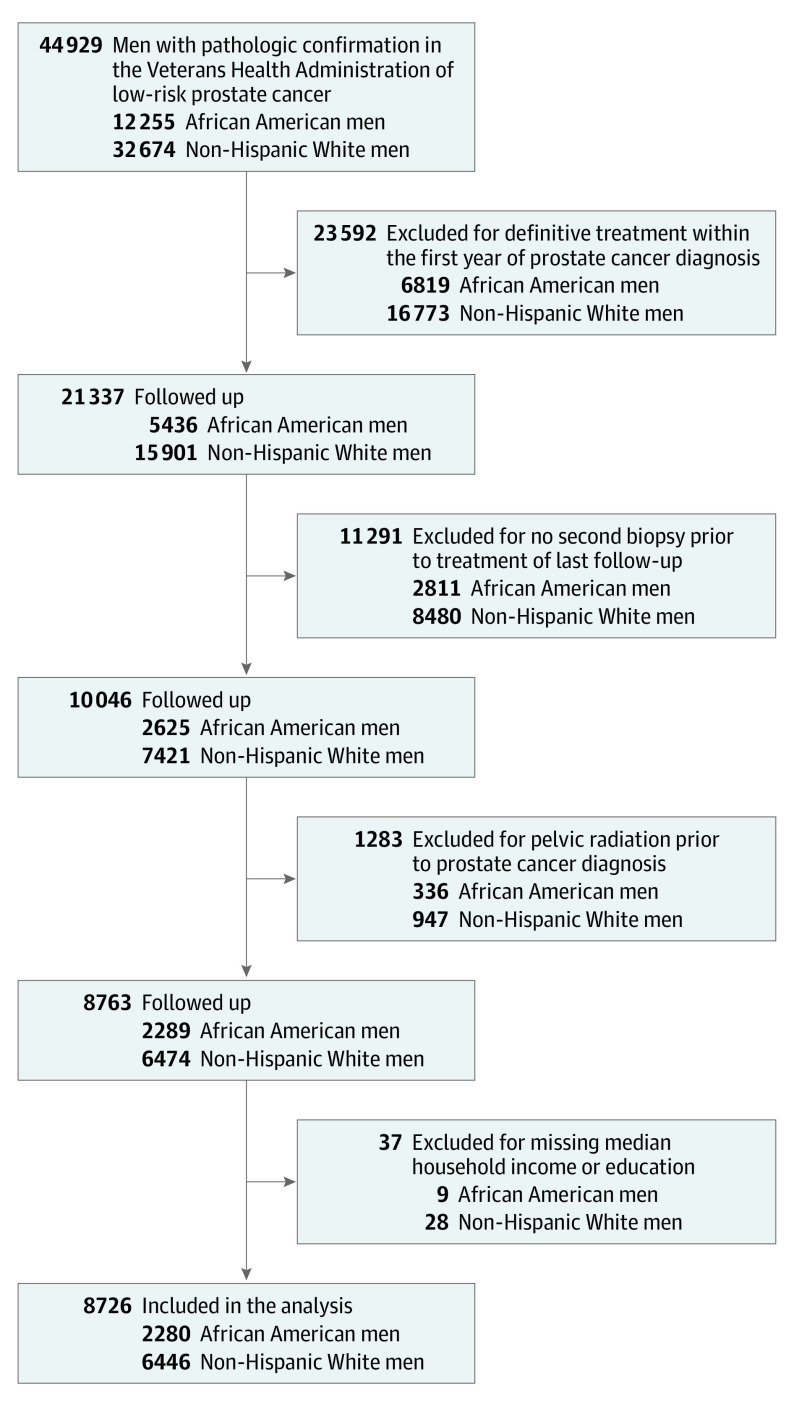
Design, setting, and participants: Retrospective cohort study in the US Veterans Health Administration Health Care System of African American and non-Hispanic White men diagnosed with low-risk prostate cancer between January 1, 2001, and December 31, 2015, and managed with active surveillance. The date of final follow-up was March 31, 2020.
Exposures: Active surveillance was defined as no definitive treatment within the first year of diagnosis and at least 1 additional surveillance biopsy.
Main outcomes and measures: Progression to at least intermediate-risk, definitive treatment, metastasis, prostate cancer-specific mortality, and all-cause mortality.
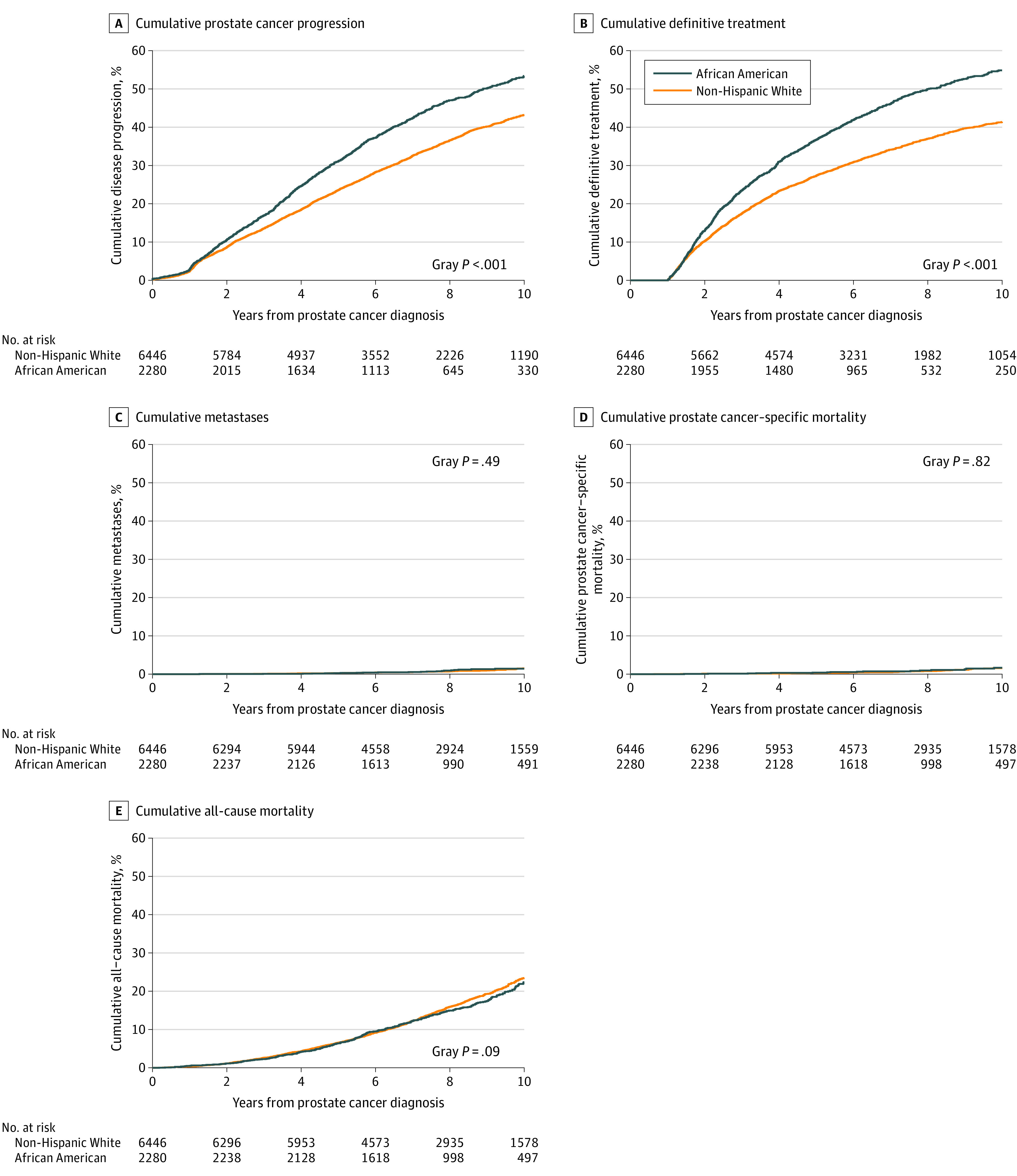
Results: The cohort included 8726 men, including 2280 African American men (26.1%) (median age, 63.2 years) and 6446 non-Hispanic White men (73.9%) (median age, 65.5 years), and the median follow-up was 7.6 years (interquartile range, 5.7-9.9; range, 0.2-19.2). Among African American men and non-Hispanic White men, respectively, the 10-year cumulative incidence of disease progression was 59.9% vs 48.3% (difference, 11.6% [95% CI, 9.2% to 13.9%); P < .001); of receipt of definitive treatment, 54.8% vs 41.4% (difference, 13.4% [95% CI, 11.0% to 15.7%]; P < .001); of metastasis, 1.5% vs 1.4% (difference, 0.1% [95% CI, -0.4% to 0.6%]; P = .49); of prostate cancer-specific mortality, 1.1% vs 1.0% (difference, 0.1% [95% CI, -0.4% to 0.6%]; P = .82); and of all-cause mortality, 22.4% vs 23.5% (difference, 1.1% [95% CI, -0.9% to 3.1%]; P = 0.09).
Conclusions and relevance: In this retrospective cohort study of men with low-risk prostate cancer followed up for a median of 7.6 years, African American men, compared with non-Hispanic White men, had a statistically significant increased 10-year cumulative incidence of disease progression and definitive treatment, but not metastasis or prostate cancer-specific mortality. Longer-term follow-up is needed to better assess the mortality risk.
Conflict of interest statement
Figures
Comment in
-
Active Surveillance for Black Men With Low-Risk Prostate Cancer.JAMA. 2020 Nov 3;324(17):1733-1734. doi: 10.1001/jama.2020.16315. JAMA. 2020. PMID: 33141193 No abstract available.
-
Socioeconomic Factors, Urological Epidemiology and Practice Patterns.J Urol. 2021 May;205(5):1505-1506. doi: 10.1097/JU.0000000000001668. Epub 2021 Feb 24. J Urol. 2021. PMID: 33625911 No abstract available.
References
-
- Mahal BA, Alshalalfa M, Spratt DE, Davicioni E, Zhao SG, Feng FY, et al. Prostate cancer genomic-risk differences between African American and White men across Gleason Scores. Eur Urol. 2019;75(6):1038-1040. - PubMed
-
- Mahal BA, Berman RA, Taplin ME, Huang FW. Prostate cancer-specific mortality across Gleason scores in black vs nonblack men. JAMA. 2018;320(23):2479-2481. - PubMed
-
- Odom BD, Mir MC, Hughes S, et al. Active surveillance for low-risk prostate cancer in African American men. Urology. 2014;83(2):364-368. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
