

Effect of tolvaptan on renal involvement in patients with autosomal dominant polycystic kidney disease according to different gene mutations
- PMID: 33141305
- PMCID: PMC7925507
- DOI: 10.1007/s10157-020-01988-4
Effect of tolvaptan on renal involvement in patients with autosomal dominant polycystic kidney disease according to different gene mutations
Abstract
Background: Autosomal dominant polycystic kidney disease (ADPKD) is an inherited disorder caused by mutations in the polycystic kidney disease (PKD) gene. Although tolvaptan has benefits for renal involvement, the different effects depending on the gene mutation type are unknown. Thus, we explore the different effects of tolvaptan on the annual changes in total kidney volume (%TKV) and estimated glomerular filtration rate (eGFR) according to the gene mutation type in ADPKD patients.
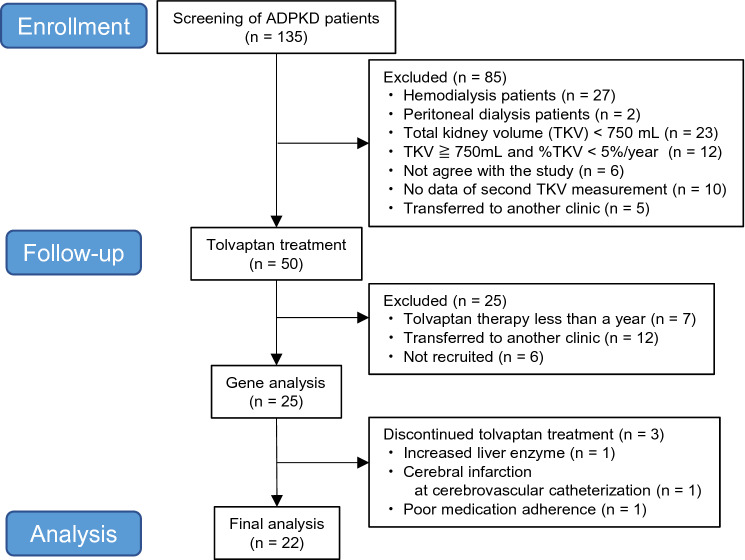
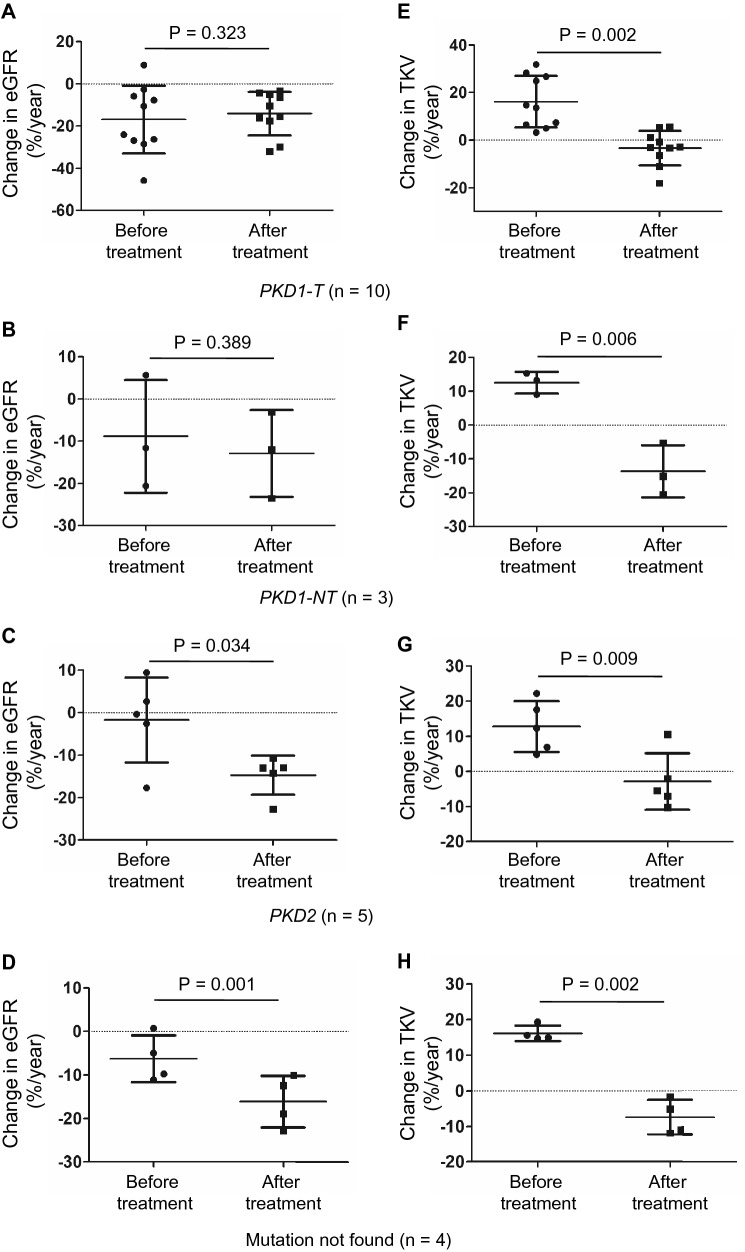
Methods: In total, 135 ADPKD patients were screened, and 22 patients taking tolvaptan for at least a year were retrospectively studied at the Kurume University Hospital. We examined the decline in renal function and %TKV by computed tomography and analyzed the gene mutation. Patients were classified into the following four groups according to gene mutation type: PKD1-truncated, PKD1-non-truncated, PKD2, and mutation not found. Patients were treated with tolvaptan, and the effects of tolvaptan were analyzed according to the gene mutation type.
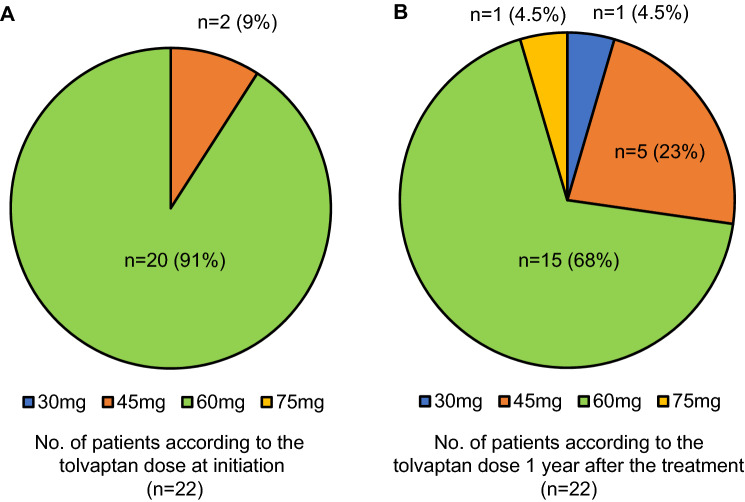
Results: Patients (age: 52.3 ± 11.2 years) were administered tolvaptan at a dose of 45 or 60 mg. No variation was observed in the annual changes in eGFR (%eGFR) (before: - 10.5% ± 13.9%, after: - 14.4% ± 8.1%, P = 0.139), whereas %TKV was significantly improved after the tolvaptan treatment (before: 14.9% ± 8.0%, after: - 5.4% ± 7.6%, P < 0.001). Unlike %eGFR, tolvaptan treatment significantly improved %TKV, regardless of the type of gene mutation.
Conclusions: A year treatment with tolvaptan significantly improved %TKV in patients with ADPKD, regardless of the gene mutation type.
Keywords: Autosomal dominant polycystic kidney disease; PKD1; PKD2; Renal function; Tolvaptan; Total kidney volume.
Conflict of interest statement
K. Fukami and T. Moriyama have received personal fees and research grant from Otsuka Pharmaceutical Co., Ltd. outside of the submitted work.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
