

Consensus Guidelines: Best Practices for Detection, Assessment and Management of Suspected Acute Drug-Induced Liver Injury During Clinical Trials in Adults with Chronic Viral Hepatitis and Adults with Cirrhosis Secondary to Hepatitis B, C and Nonalcoholic Steatohepatitis
- PMID: 33141341
- PMCID: PMC7847464
- DOI: 10.1007/s40264-020-01014-2
Consensus Guidelines: Best Practices for Detection, Assessment and Management of Suspected Acute Drug-Induced Liver Injury During Clinical Trials in Adults with Chronic Viral Hepatitis and Adults with Cirrhosis Secondary to Hepatitis B, C and Nonalcoholic Steatohepatitis
Abstract
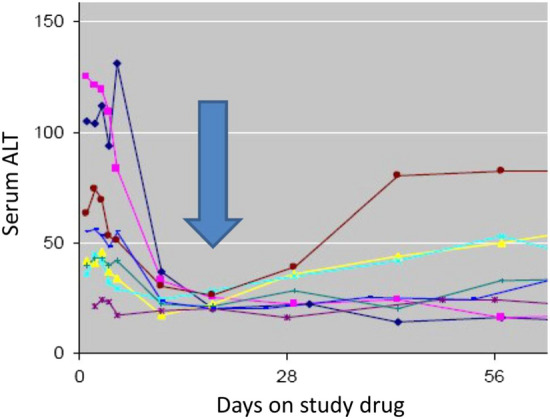
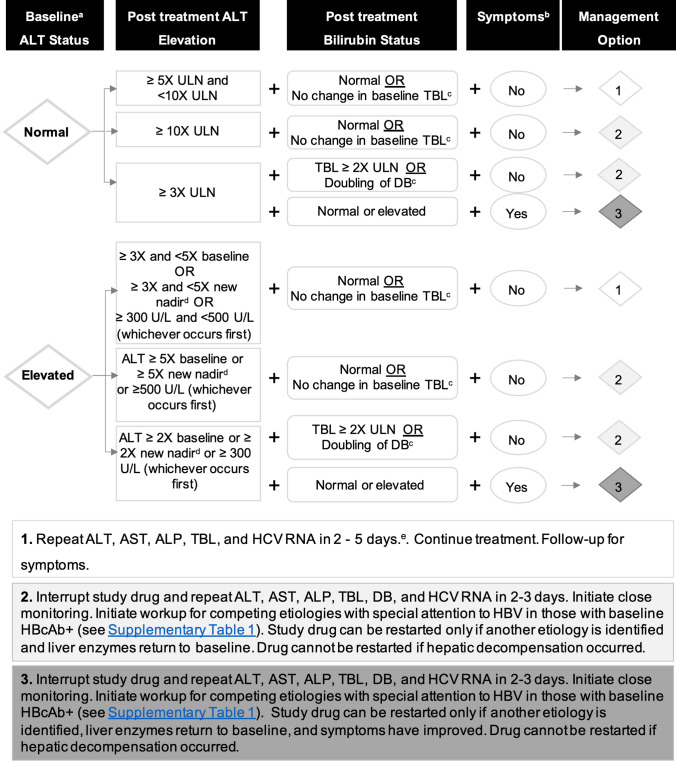
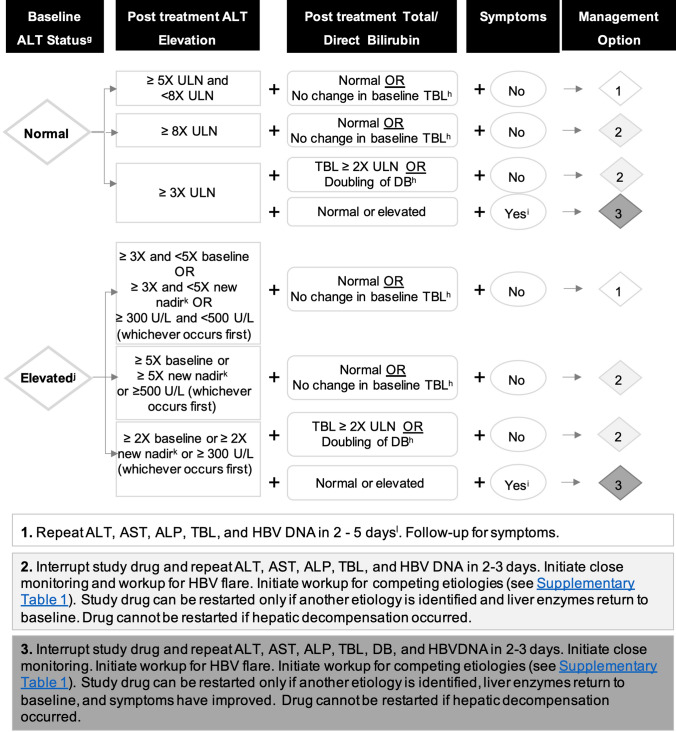
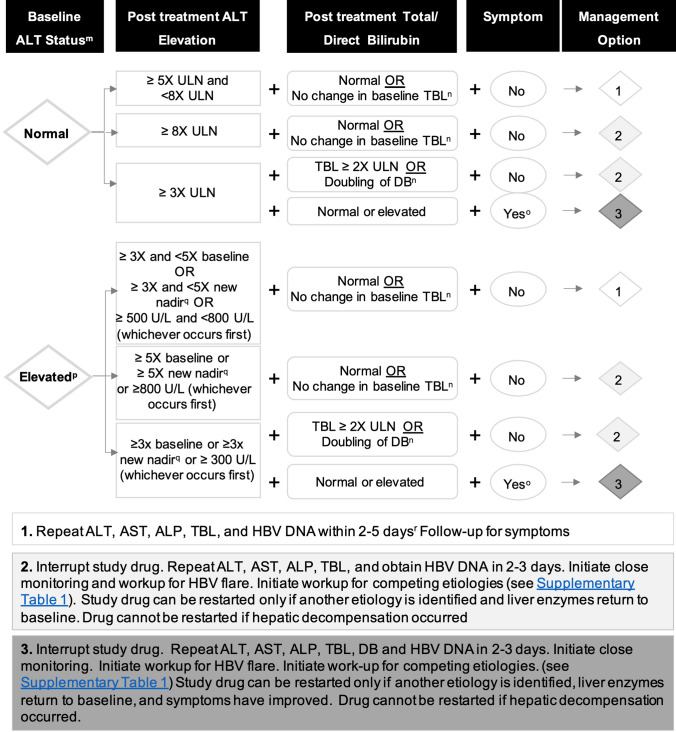
With the widespread development of new drugs to treat chronic liver diseases (CLDs), including viral hepatitis and nonalcoholic steatohepatitis (NASH), more patients are entering trials with abnormal baseline liver tests and with advanced liver injury, including cirrhosis. The current regulatory guidelines addressing the monitoring, diagnosis, and management of suspected drug-induced liver injury (DILI) during clinical trials primarily address individuals entering with normal baseline liver tests. Using the same laboratory criteria cited as signals of potential DILI in studies involving patients with no underlying liver disease and normal baseline liver tests may result in premature and unnecessary cessation of a study drug in a clinical trial population whose abnormal and fluctuating liver tests are actually due to their underlying CLD. This position paper focuses on defining best practices for the detection, monitoring, diagnosis, and management of suspected acute DILI during clinical trials in patients with CLD, including hepatitis C virus (HCV) and hepatitis B virus (HBV), both with and without cirrhosis and NASH with cirrhosis. This is one of several position papers developed by the IQ DILI Initiative, comprising members from 16 pharmaceutical companies in collaboration with DILI experts from academia and regulatory agencies. It is based on an extensive literature review and discussions between industry members and experts from outside industry to achieve consensus regarding the recommendations. Key conclusions and recommendations include (1) the importance of establishing laboratory criteria that signal potential DILI events and that fit the disease indication being studied in the clinical trial based on knowledge of the natural history of test fluctuations in that disease; (2) establishing a pretreatment value that is based on more than one screening determination, and revising that baseline during the trial if a new nadir is achieved during treatment; (3) basing rules for increased monitoring and for stopping drug for potential DILI on multiples of baseline liver test values and/or a threshold value rather than multiples of the upper limit of normal (ULN) for that test; (4) making use of more sensitive tests of liver function, including direct bilirubin (DB) or combined parameters such as aspartate transaminase:alanine transaminase (AST:ALT) ratio or model for end-stage liver disease (MELD) to signal potential DILI, especially in studies of patients with cirrhosis; and (5) being aware of potential confounders related to complications of the disease being studied that may masquerade as DILI events.
Conflict of interest statement
Drs. Chalasani, Avigan, Dimick-Santos, and Rockey have no conflicts of interest that are directly relevant to the content of this paper. Dr. Chalasani has ongoing consulting activities (or had in the preceding 12 months) with NuSirt, AbbVie, Eli Lilly, Afimmune (DS Biopharma), Allergan (Tobira), Madrigal, Shire, Axovant, Coherus, Pronova (BASF), Siemens, and Genentech. These consulting activities are generally in the areas of NAFLD and drug hepatotoxicity. Dr. Chalasani receives research grant support to his institution from Intercept, Lilly, Galectin Therapeutics, and Cumberland. Over the last decade, Dr. Chalasani has served as a paid consultant to more than 30 pharmaceutical companies, and his outside activities have regularly been disclosed to his institutional authorities. Drs. Treem, Lonjon-Domanec, Seekins, Dash, Regev, Marcinak, and Patwardhan are full-time employees of Takeda,ssen Pharmaceutica NV, Bristol Myers Squibb, Genentech, Eli Lilly, Pfizer, and AbbVie, respectively. Dr. Palmer was a full-time employee of Takeda (formerly Shire) during the drafting of this paper and is now at Liver Consulting LLC. Drs. Palmer, Lewis, and Freston serve as consultants to several pharmaceutical companies for activities related to NAFLD and DILI but have not derived any financial or other compensation from activities related to developing this best practices document. Dr. Rockey receives ongoing research grant support to his institution from Galectin Therapeutics, Genfit, Gilead Sciences, Intercept Pharmaceuticals, Mallinckrodt Pharmaceuticals, Salix Pharmaceuticals, and Sequana Pharmaceuticals. Dr. Maller was a full-time employee of Pfizer during the drafting of this paper and is now at MEMS Biopharma Consulting, LLC. Dr. Di Bisceglie serves on adjudication committees for AbbVie and Daichi Sankyo, on a data safety monitoring committee for Eiger, and as a consultant and chief medical officer to HighTide Therapeutics, which is developing a therapy for fatty liver disease. He has not derived any financial or other compensation from activities related to developing this best practices document. Dr. Andrade serves as a consultant to several pharmaceutical companies for activities related to NAFLD and DILI but has not derived any financial or other compensation from activities related to developing this best practices document.
Figures
Similar articles
-
Consensus: guidelines: best practices for detection, assessment and management of suspected acute drug-induced liver injury during clinical trials in patients with nonalcoholic steatohepatitis.Aliment Pharmacol Ther. 2019 Mar;49(6):702-713. doi: 10.1111/apt.15153. Epub 2019 Feb 13. Aliment Pharmacol Ther. 2019. PMID: 30761572 Free PMC article. Review.
-
Consensus guidelines: best practices for detection, assessment and management of suspected acute drug-induced liver injury occurring during clinical trials in adults with chronic cholestatic liver disease.Aliment Pharmacol Ther. 2020 Jan;51(1):90-109. doi: 10.1111/apt.15579. Epub 2019 Nov 25. Aliment Pharmacol Ther. 2020. PMID: 31762074 Free PMC article. Review.
-
[Guidelines for diagnosis and management of drug-induced liver injury caused by anti-tuberculosis drugs (2024 version)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Nov 12;47(11):1069-1090. doi: 10.3760/cma.j.cn112147-20240614-00338. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 39497389 Chinese.
-
Review article: Recommendations for detection, assessment and management of suspected drug-induced liver injury during clinical trials in oncology patients.Aliment Pharmacol Ther. 2024 Nov;60(10):1293-1307. doi: 10.1111/apt.18271. Epub 2024 Sep 19. Aliment Pharmacol Ther. 2024. PMID: 39300766 Review.
-
Spontaneous Fluctuations in Liver Biochemistries in Patients with Compensated NASH Cirrhosis: Implications for Drug Hepatotoxicity Monitoring.Drug Saf. 2020 Mar;43(3):281-290. doi: 10.1007/s40264-019-00896-1. Drug Saf. 2020. PMID: 31907854 Free PMC article. Clinical Trial.
Cited by
-
Opportunities and challenges in translational science.Clin Transl Sci. 2021 Sep;14(5):1629-1647. doi: 10.1111/cts.13055. Epub 2021 Jul 8. Clin Transl Sci. 2021. PMID: 33982407 Free PMC article. Review.
-
AGL9: A Novel Hepatoprotective Peptide from the Larvae of Edible Insects Alleviates Obesity-Induced Hepatic Inflammation by Regulating AMPK/Nrf2 Signaling.Foods. 2021 Aug 24;10(9):1973. doi: 10.3390/foods10091973. Foods. 2021. PMID: 34574082 Free PMC article.
-
Designing clinical trials to address alcohol use and alcohol-associated liver disease: an expert panel Consensus Statement.Nat Rev Gastroenterol Hepatol. 2024 Sep;21(9):626-645. doi: 10.1038/s41575-024-00936-x. Epub 2024 Jun 7. Nat Rev Gastroenterol Hepatol. 2024. PMID: 38849555 Free PMC article. Review.
-
Prognostic Value of Aspartate Transaminase/Alanine Transaminase Ratio in Patients With Hepatitis B Virus-Related Hepatocellular Carcinoma Undergoing Hepatectomy.Front Oncol. 2022 May 18;12:876900. doi: 10.3389/fonc.2022.876900. eCollection 2022. Front Oncol. 2022. PMID: 35664791 Free PMC article.
-
The effect of Jian Gan powder on the proliferation, migration and polarization of macrophages and relative mechanism.Pharm Biol. 2024 Dec;62(1):162-169. doi: 10.1080/13880209.2024.2309864. Epub 2024 Feb 7. Pharm Biol. 2024. PMID: 38327157 Free PMC article.
References
-
- Zimmerman HJ. Hepatotoxicity: The adverse effects of drugs and other chemicals on the liver. 2. Philadelphia: Lippincott, Williams & Wilkins; 1999.
-
- Russo MW, Watkins PB. Are patients with elevated liver tests at increased risk of drug-induced liver injury? Gastroenterology. 2004;126(5):1477–1480. - PubMed
-
- Health Canada. Guidance document: pre-market evaluation of hepatotoxicity in health products. https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/dhp-mps/alt_form....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
