

Patient-Derived Papillary Thyroid Cancer Organoids for Radioactive Iodine Refractory Screening
- PMID: 33142750
- PMCID: PMC7692469
- DOI: 10.3390/cancers12113212
Patient-Derived Papillary Thyroid Cancer Organoids for Radioactive Iodine Refractory Screening
Abstract
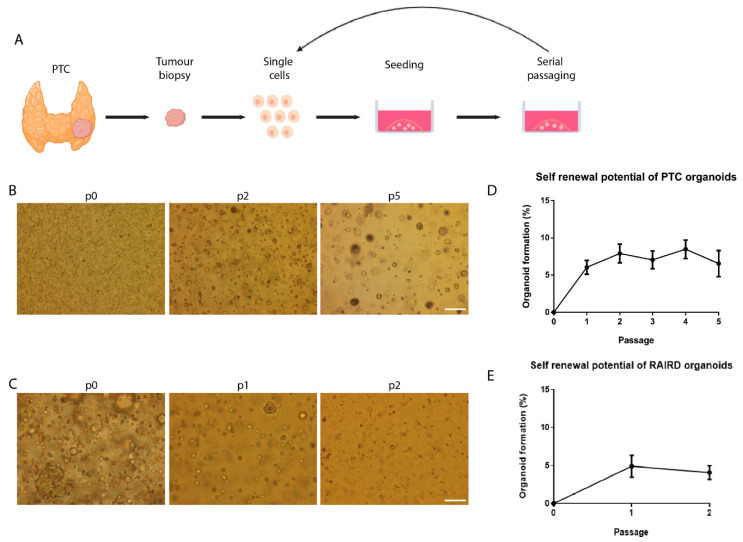
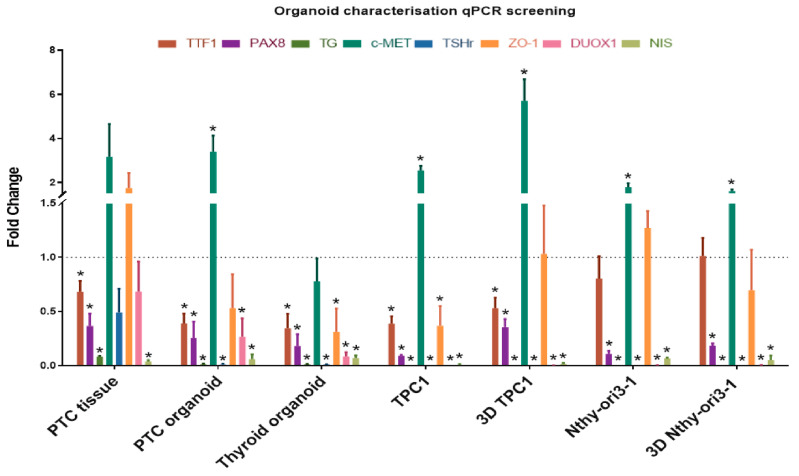
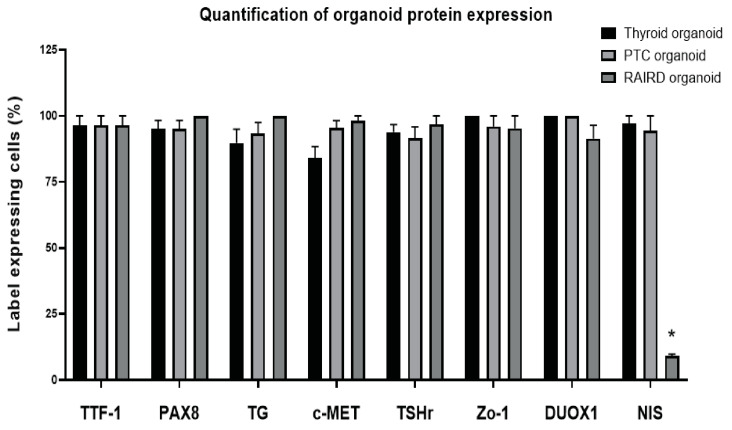
Patients with well-differentiated thyroid cancer, especially papillary thyroid cancer (PTC), are treated with surgical resection of the thyroid gland. This is followed by post-operative radioactive iodine (I131), resulting in total thyroid ablation. Unfortunately, about 15-33% of PTC patients are unable to take up I131, limiting further treatment options. The aim of our study was to develop a cancer organoid model with the potential for pre-treatment diagnosis of these I131-resistant patients. PTC tissue from thirteen patients was used to establish a long-term organoid model. These organoids showed a self-renewal potential for at least five passages, suggesting the presence of cancer stem cells. We demonstrated that thyroid specific markers, a PTC marker, and transporters/receptors necessary for iodine uptake and thyroid hormone production were expressed on a gene and protein level. Additionally, we cultured organoids from I131-resistant PTC material from three patients. When comparing PTC organoids to radioactive iodine (RAI)-refractory disease (RAIRD) organoids, a substantial discordance on both a protein and gene expression level was observed, indicating a treatment prediction potential. We showed that patient-derived PTC organoids recapitulate PTC tissue and a RAIRD phenotype. Patient-specific PTC organoids may enable the early identification of I131-resistant patients, in order to reduce RAI overtreatment and its many side effects for thyroid cancer patients.
Keywords: RAI therapy; cancer stem cells; papillary thyroid carcinoma; patient-derived tumor organoids; three-dimensional culture; treatment prediction; tumor organoids.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Husson O., Haak H.R., Van Steenbergen L.N., Nieuwlaat W.-A., Dijk B.A.C.V., Nieuwenhuijzen G.A.P., Karim-Kos H., Kuijpens J.L., Van De Poll-Franse L.V., Coebergh J.W.W. Rising incidence, no change in survival and decreasing mortality from thyroid cancer in The Netherlands since 1989. Endocr.-Relat. Cancer. 2013;20:263–271. doi: 10.1530/ERC-12-0336. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
