

Omega-3 fatty acid-containing parenteral nutrition in ICU patients: systematic review with meta-analysis and cost-effectiveness analysis
- PMID: 33143750
- PMCID: PMC7607851
- DOI: 10.1186/s13054-020-03356-w
Omega-3 fatty acid-containing parenteral nutrition in ICU patients: systematic review with meta-analysis and cost-effectiveness analysis
Abstract
Background: Omega-3 (ω-3) fatty acid (FA)-containing parenteral nutrition (PN) is associated with significant improvements in patient outcomes compared with standard PN regimens without ω-3 FA lipid emulsions. Here, we evaluate the impact of ω-3 FA-containing PN versus standard PN on clinical outcomes and costs in adult intensive care unit (ICU) patients using a meta-analysis and subsequent cost-effectiveness analysis from the perspective of a hospital operating in five European countries (France, Germany, Italy, Spain, UK) and the US.
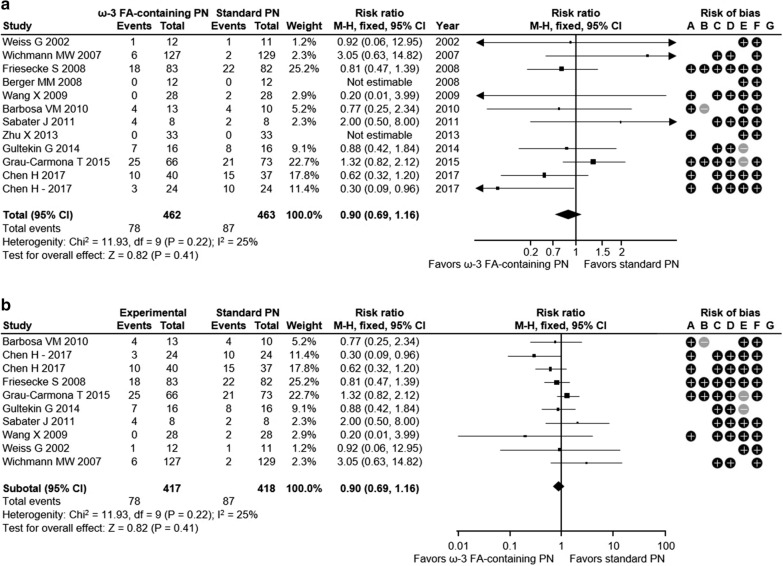
Methods: We present a pharmacoeconomic simulation based on a systematic literature review with meta-analysis. Clinical outcomes and costs comparing ω-3 FA-containing PN with standard PN were evaluated in adult ICU patients eligible to receive PN covering at least 70% of their total energy requirements and in the subgroup of critically ill ICU patients (mean ICU stay > 48 h). The meta-analysis with the co-primary outcomes of infection rate and mortality rate was based on randomized controlled trial data retrieved via a systematic literature review; resulting efficacy data were subsequently employed in country-specific cost-effectiveness analyses.
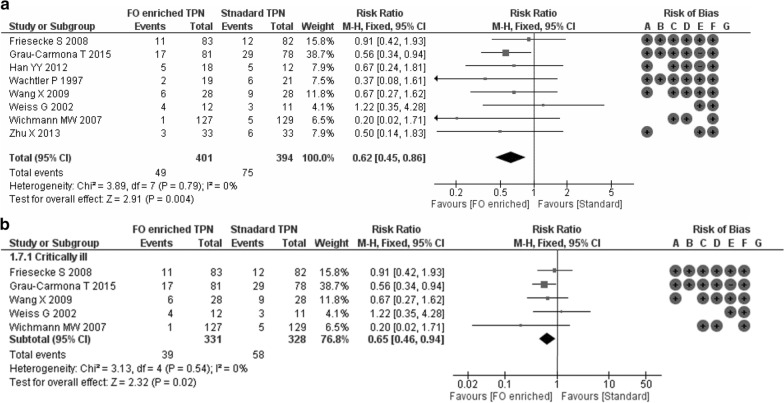
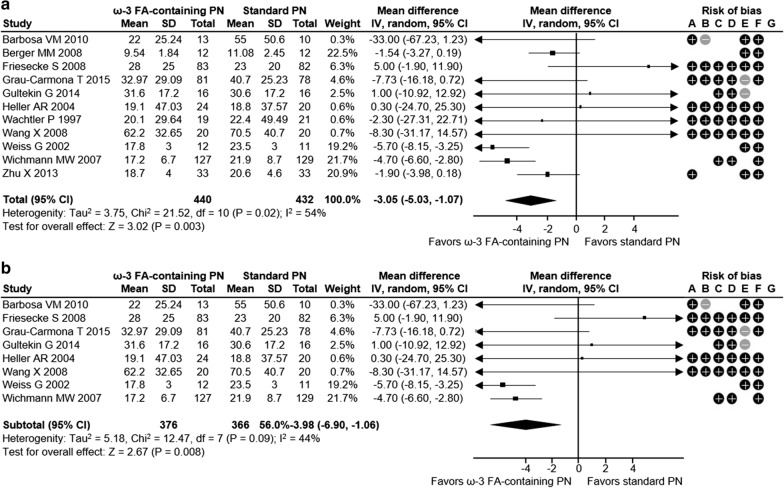
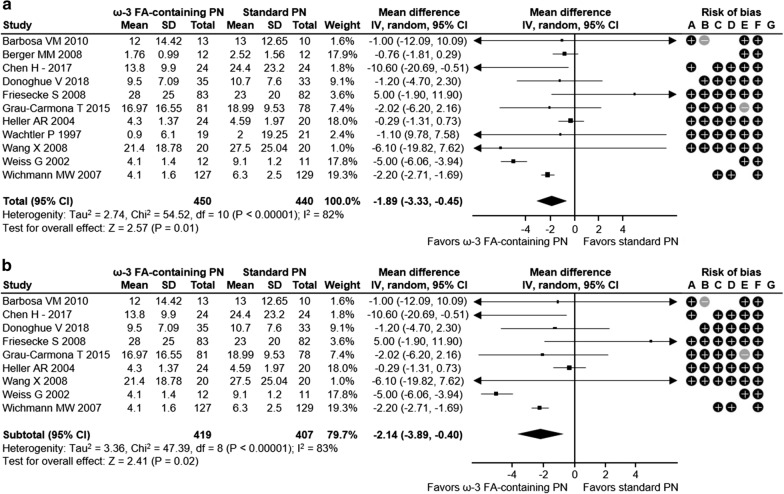
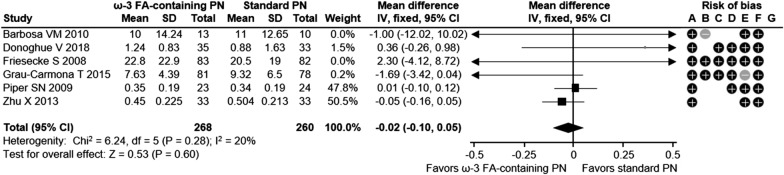
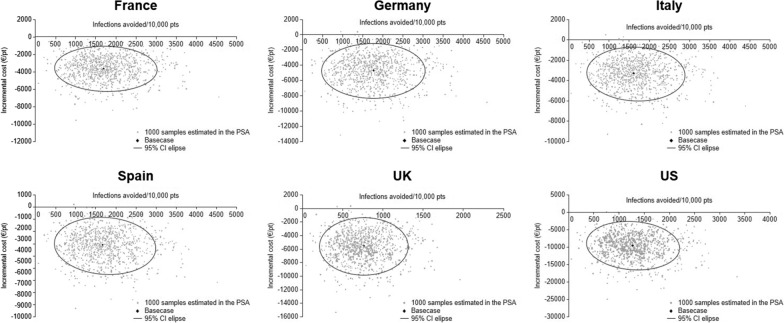
Results: In adult ICU patients, ω-3 FA-containing PN versus standard PN was associated with significant reductions in the relative risk (RR) of infection (RR 0.62; 95% CI 0.45, 0.86; p = 0.004), hospital length of stay (HLOS) (- 3.05 days; 95% CI - 5.03, - 1.07; p = 0.003) and ICU length of stay (LOS) (- 1.89 days; 95% CI - 3.33, - 0.45; p = 0.01). In critically ill ICU patients, ω-3 FA-containing PN was associated with similar reductions in infection rates (RR 0.65; 95% CI 0.46, 0.94; p = 0.02), HLOS (- 3.98 days; 95% CI - 6.90, - 1.06; p = 0.008) and ICU LOS (- 2.14 days; 95% CI - 3.89, - 0.40; p = 0.02). Overall hospital episode costs were reduced in all six countries using ω-3 FA-containing PN compared to standard PN, ranging from €-3156 ± 1404 in Spain to €-9586 ± 4157 in the US.
Conclusion: These analyses demonstrate that ω-3 FA-containing PN is associated with statistically and clinically significant improvement in patient outcomes. Its use is also predicted to yield cost savings compared to standard PN, rendering ω-3 FA-containing PN an attractive cost-saving alternative across different health care systems.
Study registration: PROSPERO CRD42019129311.
Keywords: Cost-effectiveness; Critically ill; Intensive care; Meta-analysis; Omega-3 fatty acid; Parenteral nutrition.
Conflict of interest statement
Lorenzo Pradelli: Director and employee of AdRes, which has received project funding from Fresenius. Stanislaw Klek: Speakers honoraria: Baxter, Braun, Fresenius, Nestle, Nutricia. Konstantin Mayer: Fees from Abbott, AstellasZeneca, Baxter, BBraun, Fresenius Kabi, MSD, Nestle, Novartis, Pfizer. Abdul Jabbar Omar Alsaleh: No conflicts of interest. Martin D Rosenthal: No conflicts of interest. Axel R Heller: Project funding by Fresenius-Kabi and speaker honoraria by CSL- Behring. Maurizio Muscaritoli: No conflicts of interest.
Figures

Similar articles
-
Cost-effectiveness of omega-3 fatty acid supplements in parenteral nutrition therapy in hospitals: a discrete event simulation model.Clin Nutr. 2014 Oct;33(5):785-92. doi: 10.1016/j.clnu.2013.11.016. Epub 2013 Dec 4. Clin Nutr. 2014. PMID: 24345520
-
Cost-Effectiveness of Parenteral Nutrition Containing ω-3 Fatty Acids in Hospitalized Adult Patients From 5 European Countries and the US.JPEN J Parenter Enteral Nutr. 2021 Jul;45(5):999-1008. doi: 10.1002/jpen.1972. Epub 2020 Aug 18. JPEN J Parenter Enteral Nutr. 2021. PMID: 32713007 Free PMC article.
-
ω-3 Fatty-Acid Enriched Parenteral Nutrition in Hospitalized Patients: Systematic Review With Meta-Analysis and Trial Sequential Analysis.JPEN J Parenter Enteral Nutr. 2020 Jan;44(1):44-57. doi: 10.1002/jpen.1672. Epub 2019 Jun 27. JPEN J Parenter Enteral Nutr. 2020. PMID: 31250474 Free PMC article.
-
Parenteral nutrition including an omega-3 fatty-acid-containing lipid emulsion for intensive care patients in China: a pharmacoeconomic analysis.Clinicoecon Outcomes Res. 2017 Sep 5;9:547-555. doi: 10.2147/CEOR.S139902. eCollection 2017. Clinicoecon Outcomes Res. 2017. PMID: 28919794 Free PMC article.
-
Parenteral Nutrition Containing Fish Oil for Hospitalized Non-Intensive Care Unit (ICU) Patients: A Systematic Review, Meta-Analysis, and Cost-Effectiveness Analysis.Nutrients. 2025 Apr 7;17(7):1284. doi: 10.3390/nu17071284. Nutrients. 2025. PMID: 40219041 Free PMC article.
Cited by
-
Chronic Critical Illness and PICS Nutritional Strategies.J Clin Med. 2021 May 25;10(11):2294. doi: 10.3390/jcm10112294. J Clin Med. 2021. PMID: 34070395 Free PMC article. Review.
-
Immunonutrition with Omega-3 Fatty Acid Supplementation in Severe TBI: Retrospective Analysis of Patient Characteristics and Outcomes.Res Sq [Preprint]. 2023 Nov 7:rs.3.rs-3548036. doi: 10.21203/rs.3.rs-3548036/v1. Res Sq. 2023. Update in: Neurotrauma Rep. 2024 Jun 19;5(1):574-583. doi: 10.1089/neur.2024.0005. PMID: 37986931 Free PMC article. Updated. Preprint.
-
Omega-6 sparing effects of parenteral lipid emulsions-an updated systematic review and meta-analysis on clinical outcomes in critically ill patients.Crit Care. 2022 Jan 19;26(1):23. doi: 10.1186/s13054-022-03896-3. Crit Care. 2022. PMID: 35045885 Free PMC article.
-
Parenteral nutritional support in surgical patients: expert consensus statements regarding intravenous lipid emulsions containing omega-3 fatty acids.Front Nutr. 2025 Feb 17;12:1546089. doi: 10.3389/fnut.2025.1546089. eCollection 2025. Front Nutr. 2025. PMID: 40034737 Free PMC article. Review.
-
Comprehensive quantification of C4 to C26 free fatty acids using a supercritical fluid chromatography-mass spectrometry method in pharmaceutical-grade egg yolk powders intended for total parenteral nutrition use.Anal Bioanal Chem. 2025 Mar;417(8):1461-1478. doi: 10.1007/s00216-025-05732-3. Epub 2025 Jan 23. Anal Bioanal Chem. 2025. PMID: 39849177 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
