

Leucocyte Count Does Not Improve the Diagnostic Performance of a Diagnostic Score (DS) in Distinguishing Acute Appendicitis (AA) from Nonspecific Abdominal Pain (NSAP)
- PMID: 33144440
- PMCID: PMC7811605
- DOI: 10.21873/invivo.12171
Leucocyte Count Does Not Improve the Diagnostic Performance of a Diagnostic Score (DS) in Distinguishing Acute Appendicitis (AA) from Nonspecific Abdominal Pain (NSAP)
Abstract
Background/aim: Although, acute appendicitis (AA) and nonspecific abdominal pain (NSAP) are the most common diagnoses among secondary care patients with acute abdominal pain, the diagnostic performance of leucocyte count (LC) in DS (Diagnostic Score) model is rarely considered.
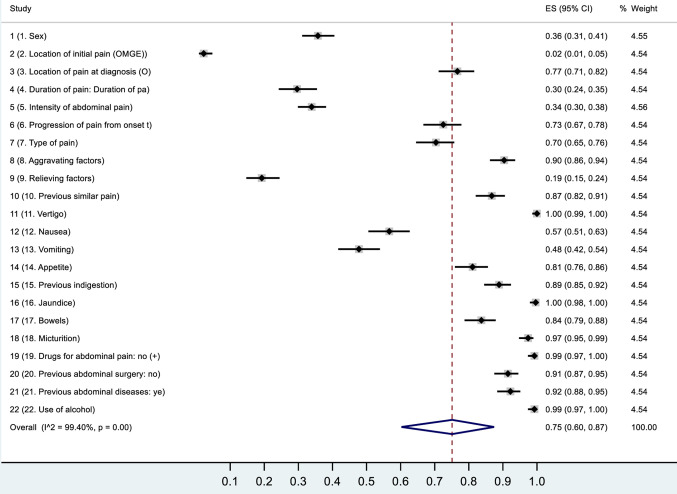
Patients and methods: As an extension of the World Organisation of Gastro-Enterology Research Committee (OMGE) acute abdominal pain study, 1,333 patients presenting with acute abdominal pain were included in the study. The clinical history and diagnostic symptoms (n=22), signs (n=14) and tests (n=3) in each patient were recorded in detail, and the collected data were related with the final diagnoses of the patients.
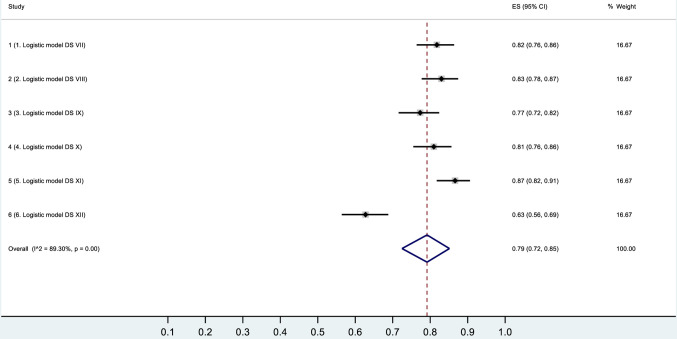
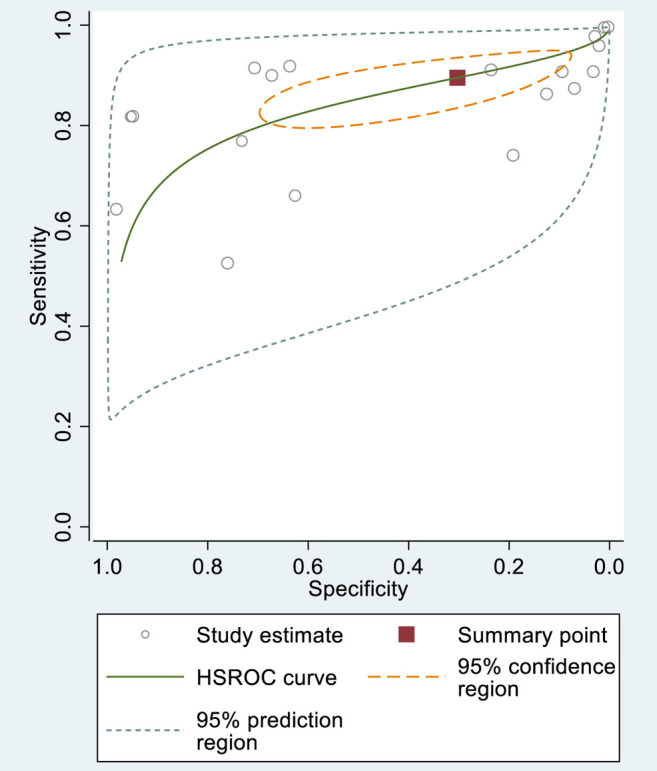
Results: In the ROC comparison test, there was no statistically significant difference in the performance of DSLC- (DS without LC) and DSLC+ (DS with LC). The highest sensitivities of the DSLC- and DSLC+ tests for detecting AA were 86% (95%CI=81-90%) and 87% (95%CI=82-91%), respectively. The highest specificities of the DSLC- and DSLC+ tests for detecting AA were 98% (95%CI=97-99%) and 98% (95%CI=96-99%), respectively.
Conclusion: DS could assist the clinician in differentiating AA from NSAP and other causes of acute abdominal pain. Importantly, LC does not improve the diagnostic performance of a DS in AA.
Keywords: Acute appendicitis; HSROC; ROC; diagnostic score; leucocyte count; non-specific abdominal pain.
Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
Conflict of interest statement
The Authors report no conflicts of interest or financial ties in relation to this study. The Authors alone are responsible for the content and writing of this article.
Figures









References
-
- De Dombal FT. The OMGE acute abdominal pain survey. Progress report 1986. Scand J Gastroenterol. 1988;23:35–42. - PubMed
-
- Eskelinen M, Ikonen J, Lipponen P. Clinical diagnosis of acute appendicitis. A prospective study of patients with acute abdominal pain. Theor Surg. 1992;7:81–85.
-
- Eskelinen M, Lipponen P. Usefulness of history-taking in non-specific abdominal pain: A prospective study of 1333 patients with acute abdominal pain in Finland. In Vivo. 2012;26:335–339. - PubMed
-
- Eskelinen M, Ikonen J, Lipponen P. Contributions of history-taking, physical examination, and computer assistance to diagnosis of acute small-bowel obstruction. A prospective study of 1333 patients with acute abdominal pain. Scand J Gastroenterol. 1994;29:715–721. doi: 10.3109/00365529409092499. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials