

Fatal and Nonfatal Events Within 14 days After Early, Intensive Mobilization Poststroke
- PMID: 33144512
- PMCID: PMC8055346
- DOI: 10.1212/WNL.0000000000011106
Fatal and Nonfatal Events Within 14 days After Early, Intensive Mobilization Poststroke
Abstract
Objective: This tertiary analysis from A Very Early Rehabilitation Trial (AVERT) examined fatal and nonfatal serious adverse events (SAEs) at 14 days.
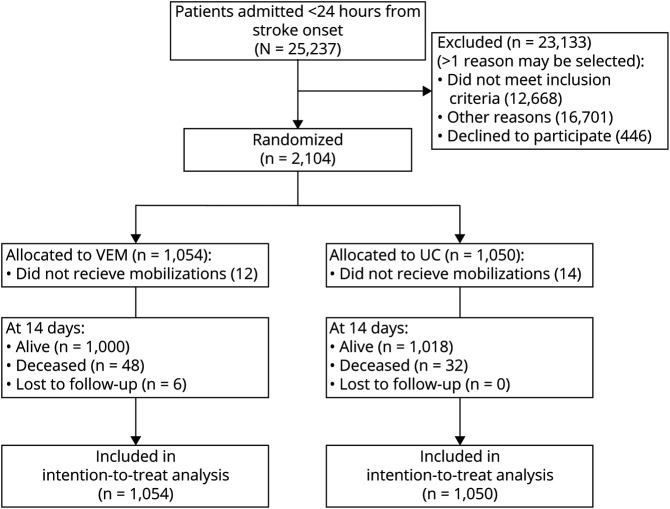
Method: AVERT was a prospective, parallel group, assessor blinded, randomized international clinical trial comparing mobility training commenced <24 hours poststroke, termed very early mobilization (VEM), to usual care (UC). Primary outcome was assessed at 3 months. Patients with ischemic or hemorrhagic stroke within 24 hours of onset were included. Treatment with thrombolytics was allowed. Patients with severe premorbid disability or comorbidities were excluded. Interventions continued for 14 days or hospital discharge if less. The primary early safety outcome was fatal SAEs within 14 days. Secondary outcomes were nonfatal SAEs classified as neurologic, immobility-related, and other. Mortality influences were assessed using binary logistic regression adjusted for baseline stroke severity (NIH Stroke Scale [NIHSS] score) and age.
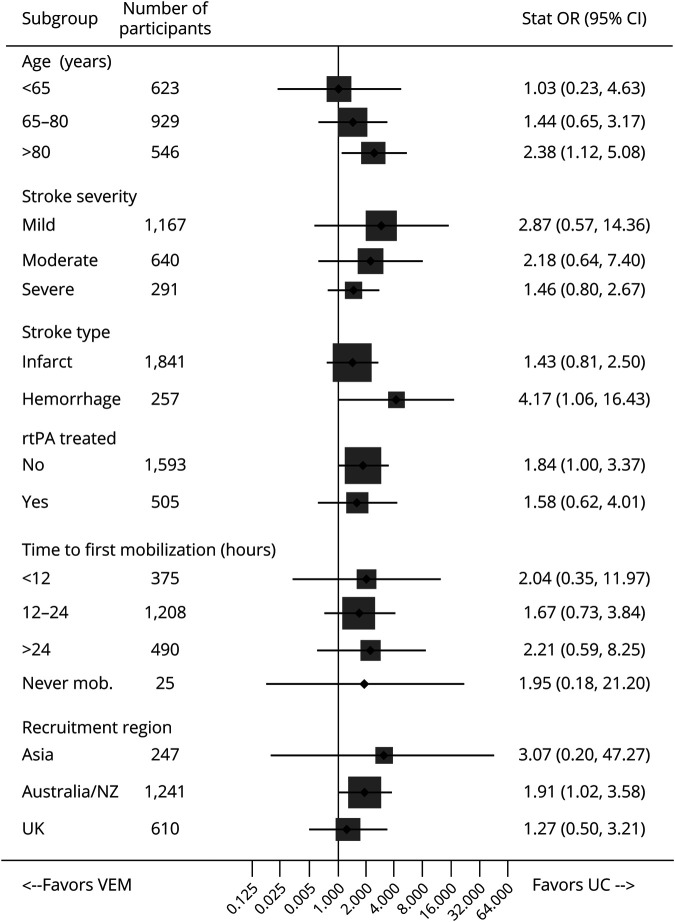
Results: A total of 2,104 participants were randomized to VEM (n = 1,054) or UC (n = 1,050) with a median age of 72 years (interquartile range [IQR] 63-80) and NIHSS 7 (IQR 4-12). By 14 days, 48 had died in VEM, 32 in UC, age and stroke severity adjusted odds ratio of 1.76 (95% confidence interval 1.06-2.92, p = 0.029). Stroke progression was more common in VEM. Exploratory subgroup analyses showed higher odds of death in intracerebral hemorrhage and >80 years subgroups, but there was no significant treatment by subgroup interaction. No difference in nonfatal SAEs was found.
Conclusion: While the overall case fatality at 14 days poststroke was only 3.8%, mortality adjusted for age and stroke severity was increased with high dose and intensive training compared to usual care. Stroke progression was more common in VEM.
Registration: Australian New Zealand Clinical Trials Registry, ACTRN12606000185561.
Classification of evidence: This study provides Class I evidence that very early mobilization increases mortality at 14 days poststroke.
© 2020 American Academy of Neurology.
Figures
Comment on
-
After a Stroke: How Quickly Should Exercise Begin?Neurology. 2021 Feb 23;96(8):e1269-e1271. doi: 10.1212/WNL.0000000000011468. Neurology. 2021. PMID: 38124243 No abstract available.
References
-
- Lynch E, Hillier S, Cadilhac D. When should physical rehabilitation commence after stroke: a systematic review. Int J Stroke 2014;9:468–478. - PubMed
-
- The AVERT Trial Collaboration Group, Bernhardt J, Langhorne P, et al. . Efficacy and safety of very early mobilisation within 24 h of stroke onset (AVERT): a randomised controlled trial. Lancet 2015;386:46–55. - PubMed
-
- Thrift AG, Thayabaranathan T, Howard G, et al. . Global stroke statistics. Int J Stroke 2017;12:13–32. - PubMed
-
- Bernhardt J, Churilov L, Dewey H, et al. . Statistical Analysis Plan (SAP) for A Very Early Rehabilitation Trial (AVERT): an international trial to determine the efficacy and safety of commencing out of bed standing and walking training (very early mobilisation) within 24 h of stroke onset vs usual stroke unit care. Int J Stroke 2015;10:23–24. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials