Endovascular Management of Direct Carotid-Cavernous Fistula: Evolution of Cost Effective Sandwich Technique
- PMID: 33144791
- PMCID: PMC7595771
- DOI: 10.1055/s-0040-1714447
Endovascular Management of Direct Carotid-Cavernous Fistula: Evolution of Cost Effective Sandwich Technique
Abstract
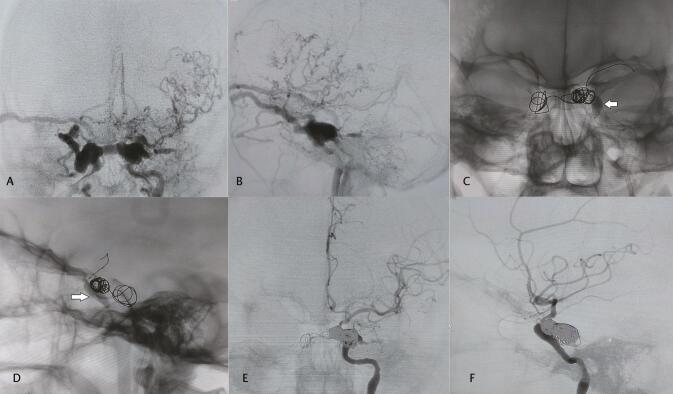
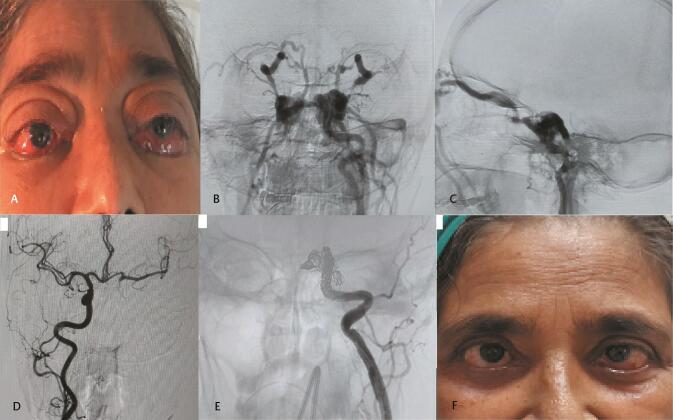
Objective There is a direct fistulous connection between the cavernous segment of the internal carotid artery and cavernous sinus in cases of direct carotid-cavernous fistula (CCF). Endovascular embolization is the mainstay of management in this condition. This study is about the evolution of endovascular treatment methods and the development of a cost-effective technique for embolization of direct CCF at a tertiary care center. Materials and Methods A retrospective analysis was performed of all the cases of direct type CCF embolized by endovascular techniques in our department from 2008 to 2018.Clinical follow-up of these patients was done at 1 week, 3 months, and 6 months. Results A total of 45 patients with 40 having a prior history of head trauma were included in this study. All cases were treated with a transarterial route except one which was treated with the transvenous approach. Detachable balloon s were used in 12 (26.67%) patients, only detachable coils in 14 cases (31.11%), both detachable balloons and coils in 9 cases (20%), and both detachable and push coils, that is, sandwich technique in 8 cases (17.78%). Parent arterial occlusion was performed in 10 patients (22.22%). There was complete resolution of chemosis and bruit in all the patients. Conclusion Endovascular treatment is the mainstay of management in direct CCF. Using more fibered thrombogenic coils in a sandwich manner decreases the cost of the treatment significantly.
Keywords: carotid cavernous fistula; detachable balloons; embolization; parent vessel occlusion; sandwich technique.
Association for Helping Neurosurgical Sick People. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. https://creativecommons.org/licenses/by-nc-nd/4.0/.
Conflict of interest statement
Conflict of Interest None declared.
Figures

References
-
- Barrow D L, Spector R H, Braun I F, Landman J A, Tindall S C, Tindall G T. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985;62(02):248–256. - PubMed
-
- Joshi D K, Singh D D, Garg D D, Singh D H, Tandon D M. Assessment of clinical improvement in patients undergoing endovascular coiling in traumatic carotid cavernous fistulas. Clin Neurol Neurosurg. 2016;149:46–54. - PubMed
-
- Williams Z R. Carotid-cavernous fistulae: a review of clinical presentation, therapeutic options, and visual prognosis. Int Ophthalmol Clin. 2018;58(02):271–294. - PubMed