

Radiological Staging of Thyroid-Associated Ophthalmopathy: Comparison of T1 Mapping with Conventional MRI
- PMID: 33144856
- PMCID: PMC7599391
- DOI: 10.1155/2020/2575710
Radiological Staging of Thyroid-Associated Ophthalmopathy: Comparison of T1 Mapping with Conventional MRI
Abstract
Background: Accurate staging of patients with thyroid-associated ophthalmopathy (TAO) is crucial for clinical decision. Full cognition of pathologic changes and staging TAO using conventional T2-weighted imaging is still limited.
Purpose: To investigate the feasibility of using T1 mapping to evaluate changes of extraocular muscles (EOMs) in TAO patients, as well as to compare T1 mapping and conventional T2-weighted imaging in staging TAO.
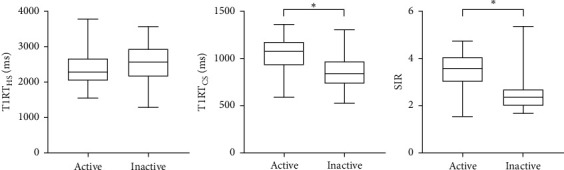
Materials and methods: Forty TAO patients were retrospectively enrolled. "Hot spot" and "cold spot" T1 relaxation times (T1RTHS and T1RTCS) of EOMs, as well as conventionally applied highest signal intensity ratio (SIR) of EOMs, were measured and compared between active and inactive groups.
Results: T1RTCS and SIR were significantly higher in active TAOs than in the inactive ones (P < 0.001), while T1RTHS was not (P=0.093). Meanwhile, T1RTCS and SIR were positively correlated with clinical activity score (r = 0.489, 0.540; P < 0.001). TIRTCS and SIR showed no significant area under curve for staging TAO (0.830 vs. 0.852; P=0.748). T1RTCS ≥ 1000 alone showed optimal staging specificity (90.0%), while integration of T1RTCS ≥ 1000 and SIR ≥ 2.9 demonstrated optimal staging efficiency and sensitivity (area under curve, 0.900; sensitivity, 86.0%).
Conclusions: Our findings suggest that the T1-mapping technique holds the potency to be utilized in TAO. The derived T1RTCS of EOMs, which may be associated with fat infiltration, could be a useful biomarker to stage the disease, serving added efficiency, sensitivity, and specificity to single usage of conventional SIR.
Copyright © 2020 Lu Chen et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures



References
LinkOut - more resources
Full Text Sources
