

Retrospective outcomes analysis of 99 consecutive uniportal awake lung biopsies: a real standard of care?
- PMID: 33145045
- PMCID: PMC7578489
- DOI: 10.21037/jtd-20-1551
Retrospective outcomes analysis of 99 consecutive uniportal awake lung biopsies: a real standard of care?
Abstract
Background: Surgical lung biopsy for interstitial lung disease (ILD) is traditionally performed through video-assisted thoracic surgery (VATS) and general anesthesia (GA). The mortality and morbidity rates associated with this procedure are not negligible, especially in patients with significant risk factors and respiratory impairment. Based on these considerations, our center evaluated a safe non-intubated VATS approach for lung biopsy performed in ILD subjects.
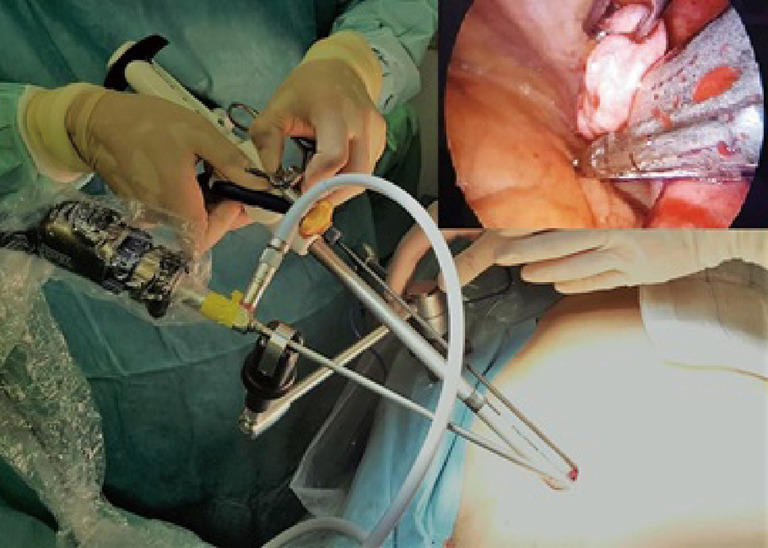
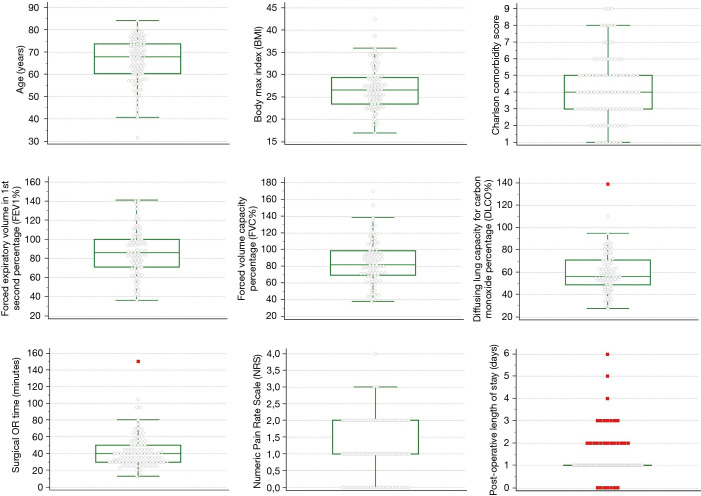
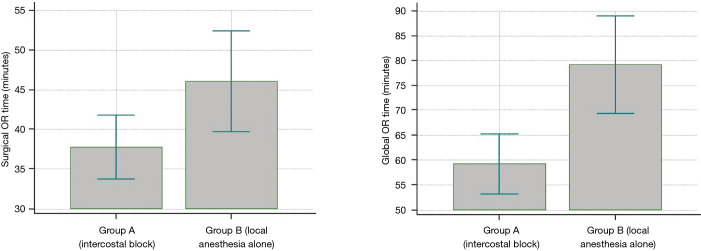
Methods: Ninety-nine patients affected by undetermined ILD were enrolled in a retrospective cohort study. In all instances, lung biopsies were performed using a non-intubated VATS technique, in spontaneously breathing patients, with or without intercostal nerve blockage. The primary end-point was the diagnostic yield, while surgical and global operating room times, post-operative length of stay (pLOS), numeric pain rating scale (NPRS) after surgery and early mortality were considered as secondary outcomes.
Results: All the procedures were carried out without conversion to GA. The pathological diagnosis was achieved in 97 patients with a diagnostic yield of 98%. The mean operating room length-of-stay and operating time were 73.7 and 42.5 min, respectively. Mean pLOS was 1.3 days with a low readmissions rate (3%). No mortality in the first 30 days due to acute exacerbation of ILD occurred. Both analgesia methods resulted in optimal feasibility with a mean NPRS score of 1.13.
Conclusions: In undetermined ILD patients, surgical lung biopsy with a non-intubated VATS approach and spontaneous ventilation anesthesia appears to be both a practical and safe technique with an excellent diagnostic yield and high level of patient satisfaction.
Keywords: Awake surgery; interstitial lung disease (ILD); non-intubated video-assisted thoracic surgery (NIVATS); surgical lung biopsy (SLB); tubeless anesthesia.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd-20-1551). The authors have no conflicts of interest to declare.
Figures

References
LinkOut - more resources
Full Text Sources