

Thyroid cancer diagnosis in the era of precision imaging
- PMID: 33145090
- PMCID: PMC7578495
- DOI: 10.21037/jtd.2019.08.37
Thyroid cancer diagnosis in the era of precision imaging
Abstract
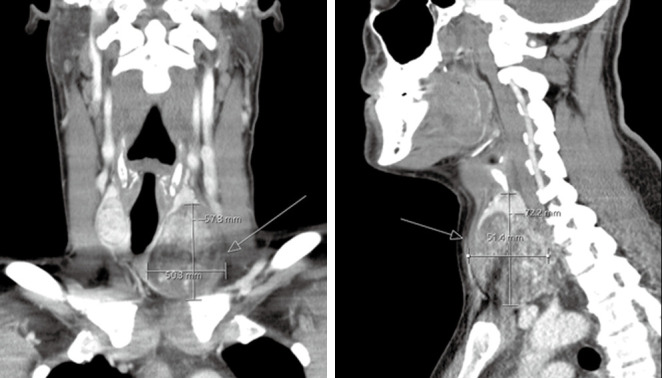
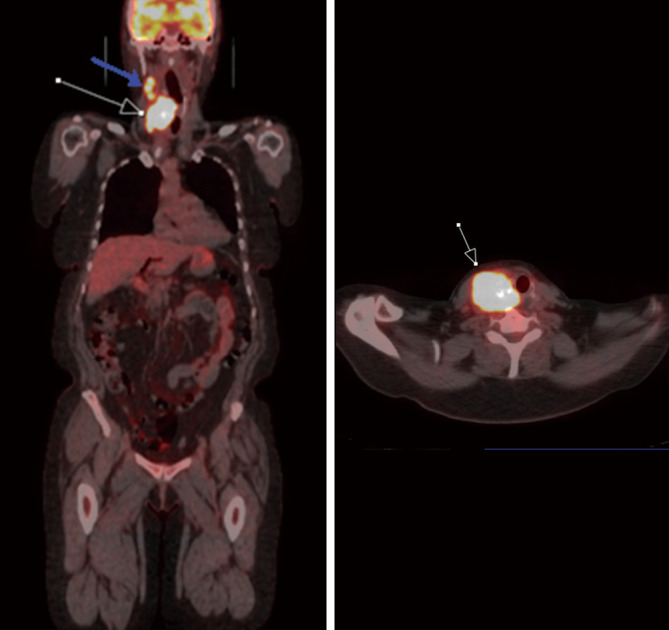
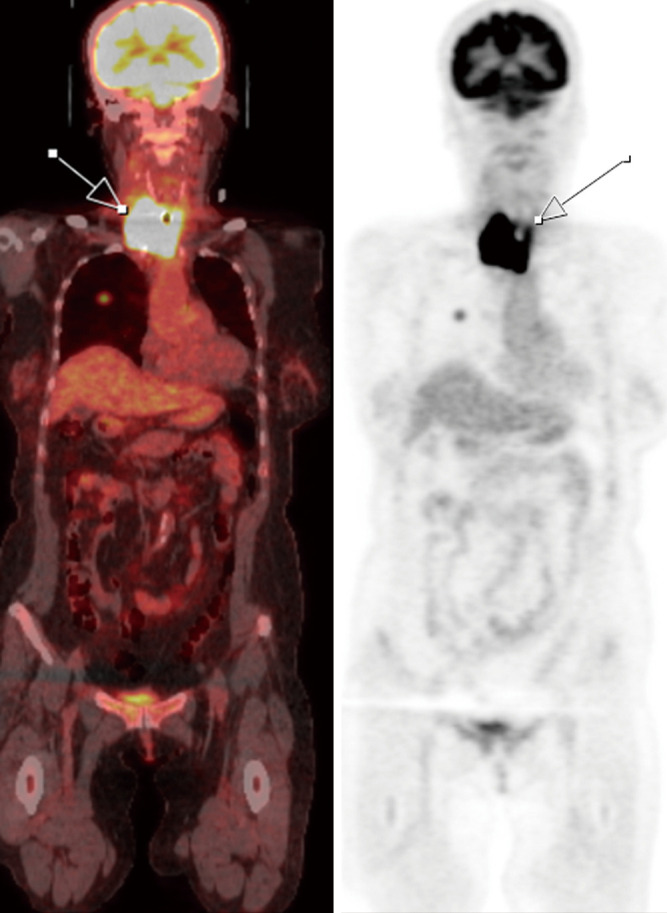
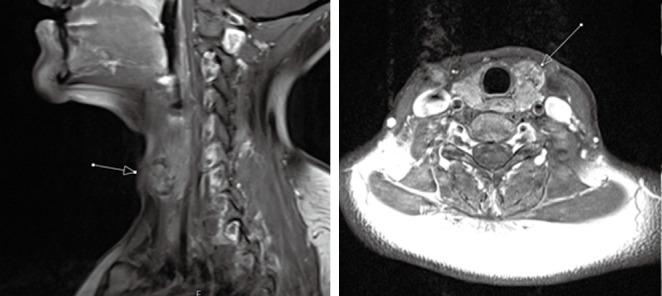
Thyroid cancer affects 1.3% of the population with increasing rates of incidence over the last decade (approximately 2% per year). Although the overall prognosis is good in the differentiated subtypes, there has been a slow but steady increase in rate of deaths associated with thyroid cancer (approximately 0.7% per year over the last decade). Thyroid cancer is usually detected when: (I) patients feel a lump in the neck; (II) a routine clinical exam is performed; (III) an incidental thyroid nodule is identified on diagnostic imaging (e.g., CT neck or chest, carotid ultrasound, PET scan acquired for non-thyroid pathology). Identification of suspicious thyroid nodules results in further diagnostic work-up including laboratory assessment, further imaging, and biopsy. Accurate diagnosis is required for clinical staging and optimal patient treatment design. In this review, we aim to discuss utility of various imaging modalities and their role in thyroid cancer diagnosis and management. Additionally, we aim to highlight emerging diagnostic techniques that aim to improve diagnostic specificity and accuracy in thyroid cancer, thus paving way for precision medicine.
Keywords: Positron emission tomography/computed tomography (PET/CT); cancer; magnetic resonance imaging (MRI); thyroid; ultrasound.
2020 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd.2019.08.37). The series “Role of Precision Imaging in Thoracic Disease” was commissioned by the editorial office without any funding or sponsorship. AC served as the unpaid Guest Editor for the series. The other authors have no other conflicts of interest to declare.
Figures
References
-
- Shore SL. Thyroid Cancer. In: Vinjamuri S, editor. PET/CT in Thyroid Cancer. Cham: Springer International Publishing; 2018. p. 1-7.
-
- Shore SL. Thyroid Cancer Pathology. In: Vinjamuri S, editor. PET/CT in Thyroid Cancer. Cham: Springer International Publishing; 2018. p. 9-13.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources