

Closure of Skull Base Defects after Endonasal Endoscopic Resection of Planum Sphenoidale and Tuberculum Sellae Meningiomas
- PMID: 33145222
- PMCID: PMC7591213
- DOI: 10.4103/ajns.AJNS_62_20
Closure of Skull Base Defects after Endonasal Endoscopic Resection of Planum Sphenoidale and Tuberculum Sellae Meningiomas
Abstract
Background: The expanded endoscopic endonasal transplanum transtuberculum approach allows tumor removal by minimally invasive procedures. A large dural and bone defect is created during the surgical procedure, increasing the risk of postoperative cerebrospinal fluid (CSF) leakage.
Objective: The aim of this study is to describe a surgical technique and complications observed in patients undergoing endonasal resection of planum sphenoidale and/or tuberculum sellae meningiomas.
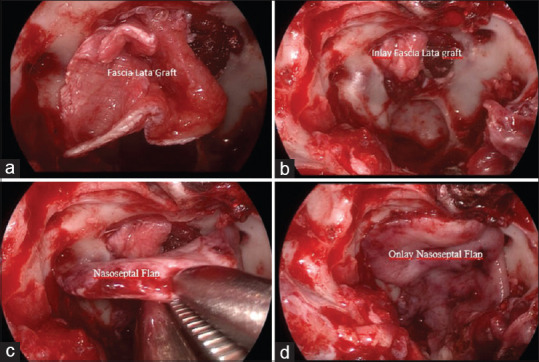
Methods: A retrospective analysis was performed of patients with planum sphenoidale and/or tuberculum sellae meningiomas after expanded endoscopic endonasal resection between June 2013 and August 2018, in which autologous grafts, fascia lata inlay, and nasoseptal flap onlay were used for closure of skull base defects.
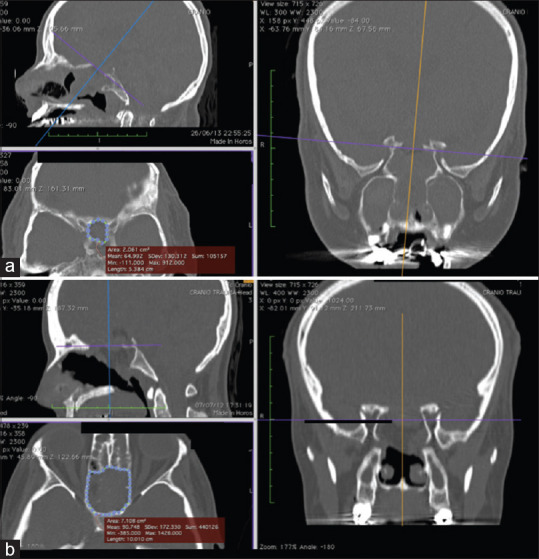
Results: Ten patients were included in the analysis. No cases of postoperative CSF leakages or meningitis were reported, whereas two patients evolved with postoperative infectious complications (fungal ball in right frontal sinus and brain abscess). The skull base defect created for resection measured, on average, 3.58 cm2.
Conclusion: Our experience suggests that closure of skull base defects using combined fascia lata inlay and nasoseptal flap onlay is effective for preventing postoperative CSF leakage in resection of planum sphenoidale and/or tuberculum sellae meningiomas, and offers high reproducibility due to its low cost.
Keywords: Cerebrospinal fluid leak; meningioma; skull base; surgical flaps.
Copyright: © 2020 Asian Journal of Neurosurgery.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Endoscopic Endonasal Transsphenoidal Approach for Resection of Tuberculum Sella and Planum Sphenoidale Meningiomas: A Snapshot of Our Institutional Experience.Asian J Neurosurg. 2020 Feb 25;15(1):22-25. doi: 10.4103/ajns.AJNS_85_19. eCollection 2020 Jan-Mar. Asian J Neurosurg. 2020. PMID: 32181168 Free PMC article.
-
Aggressive resection of craniopharyngioma achieved by drilling the tuberculum sellae/planum sphenoidale using a frontal basal interhemispheric approach: A review of 55 cases.J Clin Neurosci. 2021 Jan;83:13-20. doi: 10.1016/j.jocn.2020.11.042. Epub 2020 Dec 14. J Clin Neurosci. 2021. PMID: 33328148
-
Challenges and surgical nuances in reconstruction of large planum sphenoidale tuberculum sellae defects after endoscopic endonasal resection of parasellar skull base tumors.Laryngoscope. 2013 Jun;123(6):1353-60. doi: 10.1002/lary.23766. Epub 2013 Mar 11. Laryngoscope. 2013. PMID: 23483459
-
Endoscopic endonasal versus open transcranial resection of anterior midline skull base meningiomas.World Neurosurg. 2012 May-Jun;77(5-6):713-24. doi: 10.1016/j.wneu.2011.08.025. Epub 2011 Nov 7. World Neurosurg. 2012. PMID: 22120296 Review.
-
An Overview of Anterior Skull Base Meningiomas and the Endoscopic Endonasal Approach.Otolaryngol Clin North Am. 2016 Feb;49(1):141-52. doi: 10.1016/j.otc.2015.08.002. Otolaryngol Clin North Am. 2016. PMID: 26614834 Review.
References
-
- Cappabianca P, Alfieri A, de Divitiis E. Endoscopic endonasal transsphenoidal approach to the sella: Towards functional endoscopic pituitary surgery (FEPS) Minim Invasive Neurosurg. 1998;41:66–73. - PubMed
-
- Kassam A, Snyderman CH, Mintz A, Gardner P, Carrau RL. Expanded endonasal approach: The rostrocaudal axis Part I Crista galli to the sella turcica. Neurosurg Focus. 2005;19:E3. - PubMed
-
- Kassam A, Snyderman CH, Mintz A, Gardner P, Carrau RL. Expanded endonasal approach: The rostrocaudal axis Part II Posterior clinoids to the foramen magnum. Neurosurg Focus. 2005;19:E4. - PubMed
-
- Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R. Expanded endonasal approach: Fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus. 2005;19:E6. - PubMed
-
- Stamm AM. Transnasal endoscopy-assisted skull base surgery. Ann Otol Rhinol Laryngol Suppl. 2006;196:45–53. - PubMed