

The utility of emergency department physical therapy and case management consultation in reducing hospital admissions
- PMID: 33145536
- PMCID: PMC7593441
- DOI: 10.1002/emp2.12075
The utility of emergency department physical therapy and case management consultation in reducing hospital admissions
Abstract
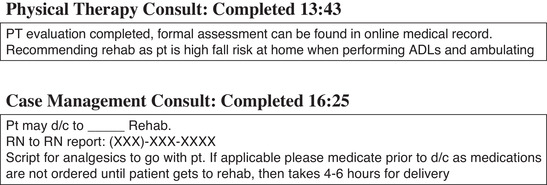
Background: A significant number of patients who present to the emergency department (ED) following a fall or with other injuries require evaluation by a physical therapist. Traditionally, once emergent conditions are excluded in the ED, these patients are admitted to the hospital for evaluation by a physical therapist to determine whether they should be transferred to a sub-acute rehabilitation facility, discharged, require services at home, or require further inpatient care. Case management is typically used in conjunction with a physical therapist to determine eligibility for recommended services and to aid in placement.
Objective: To evaluate the benefit of using ED-based physical therapist and case management services in lieu of routine hospital admission.
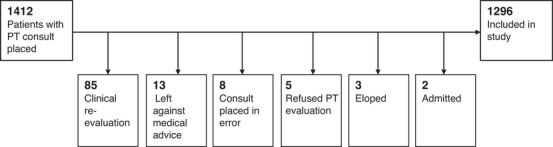
Methods: Retrospective, observational study of consecutive patients presenting to an urban, tertiary care academic medical center ED between December 1, 2017, and November 30, 2018, who had a physical therapist consult placed in the ED. We additionally evaluated which of these patients were placed into ED observation for physical therapist consultation, how many required case management, and ED disposition: discharged home from the ED or ED observation with or without services, placed in a rehabilitation facility, or admitted to the hospital.
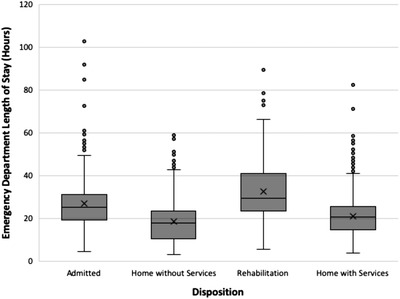
Results: During the 12-month study period, 1296 patients (2.4% of the total seen in the ED) were assessed by a physical therapist. The mean age was 75.5 ± 15.2 and 832 (64.2%) were female. Case management was involved in 91.8% of these cases. The final patient disposition was as follows: admission 24.3% (95% CI = 22.1-26.7%), home discharge with or without services 47.8% (95% CI = 45.1-50.5%), rehabilitation (rehab) setting 27.9% (95% CI = 25.6%-30.4). The median (interquartile range) time in observation was 13.1 (6.0-20.3), 9.9 (1.8-15.8), and 18.4 (14.1-24.8) hours for patients admitted, discharged home, or sent to rehabilitation (P < 0.001). Among the 979 patients discharged home or sent to rehabilitation, 17 (1.7%) returned to the ED within 72 hours and were ultimately admitted.
Conclusion: Given that the standard of care would otherwise be an admission to the hospital for 1 day or more for all patients requiring physical therapist consultation, an ED-based physical therapy and case management system serves as a viable method to substantially decrease hospital admissions and potentially reduce resource use, length of hospital stay, and cost both to patients and the health care system.
Keywords: case management; hospital admission reduction; observation units; pathways; physical therapy; rehabilitation placement.
© 2020 The Authors. JACEP Open published by Wiley Periodicals LLC on behalf of the American College of Emergency Physicians.
Figures
Similar articles
-
Who is less likely to die in association with improved National Emergency Access Target (NEAT) compliance for emergency admissions in a tertiary referral hospital?Aust Health Rev. 2016 Apr;40(2):149-154. doi: 10.1071/AH14242. Aust Health Rev. 2016. PMID: 26278814
-
An Emergency Department Observation Unit Is a Feasible Setting for Multidisciplinary Geriatric Assessments in Compliance With the Geriatric Emergency Department Guidelines.Acad Emerg Med. 2018 Jan;25(1):76-82. doi: 10.1111/acem.13328. Epub 2017 Nov 24. Acad Emerg Med. 2018. PMID: 28975679 Free PMC article.
-
A randomized trial of home oxygen therapy from the emergency department for acute bronchiolitis.Pediatrics. 2006 Mar;117(3):633-40. doi: 10.1542/peds.2005-1322. Pediatrics. 2006. PMID: 16510641 Clinical Trial.
-
Evaluating mental health decision units in acute care pathways (DECISION): a quasi-experimental, qualitative and health economic evaluation.Health Soc Care Deliv Res. 2023 Dec;11(25):1-221. doi: 10.3310/PBSM2274. Health Soc Care Deliv Res. 2023. PMID: 38149657
-
Caseworker-assigned discharge plans to prevent hospital readmission for acute exacerbations in children with chronic respiratory illness.Cochrane Database Syst Rev. 2018 Nov 2;11(11):CD012315. doi: 10.1002/14651858.CD012315.pub2. Cochrane Database Syst Rev. 2018. PMID: 30387126 Free PMC article.
Cited by
-
It's time to mobilize: Moving mobility interventions for delirium from inpatient units to the emergency department.J Am Coll Emerg Physicians Open. 2023 Feb 6;4(1):e12900. doi: 10.1002/emp2.12900. eCollection 2023 Feb. J Am Coll Emerg Physicians Open. 2023. PMID: 36776215 Free PMC article. No abstract available.
-
Reply to Moretti et al. Would Moving Forward Mean Going Back? Comment on "Maselli et al. Direct Access to Physical Therapy: Should Italy Move Forward? Int. J. Environ. Res. Public Health 2022, 19, 555".Int J Environ Res Public Health. 2022 Apr 12;19(8):4620. doi: 10.3390/ijerph19084620. Int J Environ Res Public Health. 2022. PMID: 35457488 Free PMC article.
-
On-site physiotherapy in older emergency department patients following a fall: a randomized controlled trial.Eur Geriatr Med. 2025 Feb;16(1):205-217. doi: 10.1007/s41999-024-01091-x. Epub 2024 Nov 16. Eur Geriatr Med. 2025. PMID: 39548032 Free PMC article. Clinical Trial.
-
Direct Access to Physical Therapy: Should Italy Move Forward?Int J Environ Res Public Health. 2022 Jan 4;19(1):555. doi: 10.3390/ijerph19010555. Int J Environ Res Public Health. 2022. PMID: 35010817 Free PMC article.
-
Emergency Department-Based Physical Function Measures for Falls in Older Adults and Outcomes: A Secondary Analysis of GAPcare.J Geriatr Phys Ther. 2024 Apr 24:10.1519/JPT.0000000000000403. doi: 10.1519/JPT.0000000000000403. Online ahead of print. J Geriatr Phys Ther. 2024. PMID: 38656264
References
-
- Sheehy A, Caponi B, Gangireddy S, et al. Observation and inpatient status: clinical impact of the 2‐midnight rule. J Hosp Med. 2014;0(4):203‐209. - PubMed
-
- Capp R, Sun B, Boatright D, Gross C. The impact of emergency department observation units on United States emergency department admission rates. J Hosp Med. 2015;10(11): 738‐742. - PubMed
-
- Cheng AHY, Barclay NG, Abu‐Laban RB. Effect of a multi‐diagnosis observation unit on emergency department length of stay and inpatient admission rate at two Canadian hospitals. J Emerg Med. 2016;1(6):739‐747. - PubMed
-
- Brillman J, Mathers‐Dunbar L, Graff L, et al. Management of observation units. Ann Emerg Med. 1995;25(6):823‐830. - PubMed
-
- Roberts RR, Zalenski RJ, Mensah EK, et al. Costs of an emergency department‐based accelerated diagnostic protocol vs. hospitalization in patients with chest pain: a randomized controlled trial. JAMA. 1997;278(20):1670‐1676. - PubMed
LinkOut - more resources
Full Text Sources