

Blood neurofilament light: a critical review of its application to neurologic disease
- PMID: 33146954
- PMCID: PMC7732243
- DOI: 10.1002/acn3.51234
Blood neurofilament light: a critical review of its application to neurologic disease
Abstract
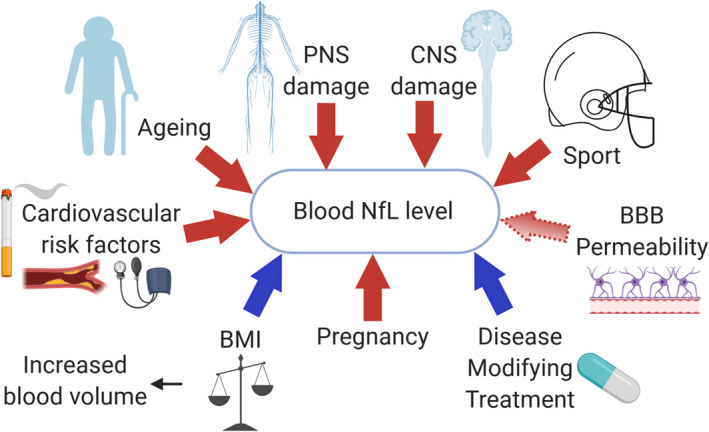
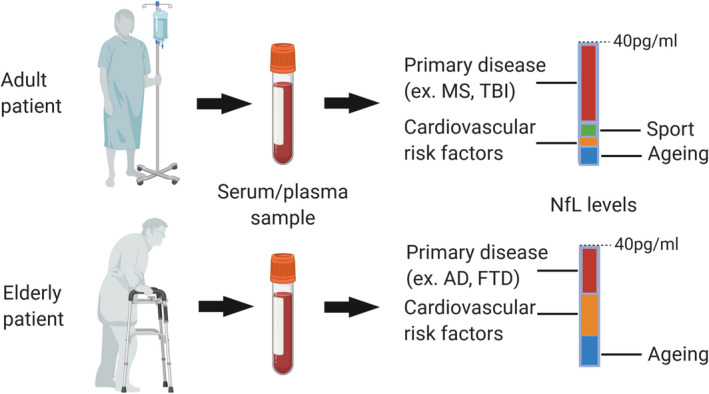
Neuronal injury is a universal event that occurs in disease processes that affect both the central and peripheral nervous systems. A blood biomarker linked to neuronal injury would provide a critical measure to understand and treat neurologic diseases. Neurofilament light chain (NfL), a cytoskeletal protein expressed only in neurons, has emerged as such a biomarker. With the ability to quantify neuronal damage in blood, NfL is being applied to a wide range of neurologic conditions to investigate and monitor disease including assessment of treatment efficacy. Blood NfL is not specific for one disease and its release can also be induced by physiological processes. Longitudinal studies in multiple sclerosis, traumatic brain injury, and stroke show accumulation of NfL over days followed by elevated levels over months. Therefore, it may be hard to determine with a single measurement when the peak of NfL is reached and when the levels are normalized. Nonetheless, measurement of blood NfL provides a new blood biomarker for neurologic diseases overcoming the invasiveness of CSF sampling that restricted NfL clinical application. In this review, we examine the use of blood NfL as a biologic test for neurologic disease.
© 2020 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
CB has nothing to disclose. CT received personal compensation for advisory board/consulting for Biogen‐Idec, Merck Serono, Novartis, Sanofi, Bayer, Celgene, Alexion, and received financial support for research activities from Merck Serono and Novartis Pharmaceuticals. HLW reports grants from National Institutes of Health, National Multiple Sclerosis Society, Verily Life Sciences, Google Life Sciences, EMD Serono, Inc., Biogen, Teva Pharmaceuticals, and Novartis; grants and consulting fees from Sanofi US Services, Inc. and Genentech, Inc.; consulting and advising fees from Tilos Therapeutics; consulting and advising fees from Tiziana Life Sciences; consulting and advising fees from IM Therapeutics; personal, consulting, and advising fees from vTv Therapeutics; personal, consulting, and advising fees from MedDay Pharmaceuticals.
Figures
References
-
- Khalil M, Teunissen CE, Otto M, et al. Neurofilaments as biomarkers in neurological disorders. Nat Rev Neurol 2018;14:577–589. - PubMed
-
- van Lieverloo GGA, Wieske L, Verhamme C, et al. Serum neurofilament light chain in chronic inflammatory demyelinating polyneuropathy. J Peripher Nerv Syst 2019;24:187–194. - PubMed
-
- Rosengren LE, Karlsson JE, Karlsson JO, et al. Patients with amyotrophic lateral sclerosis and other neurodegenerative diseases have increased levels of neurofilament protein in CSF. J. Neurochem 1996;67:2013–2018. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical