

Dydrogesterone as an oral alternative to vaginal progesterone for IVF luteal phase support: A systematic review and individual participant data meta-analysis
- PMID: 33147288
- PMCID: PMC7641447
- DOI: 10.1371/journal.pone.0241044
Dydrogesterone as an oral alternative to vaginal progesterone for IVF luteal phase support: A systematic review and individual participant data meta-analysis
Abstract
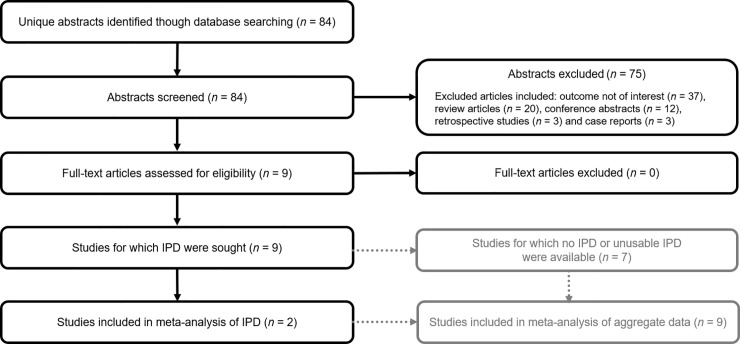
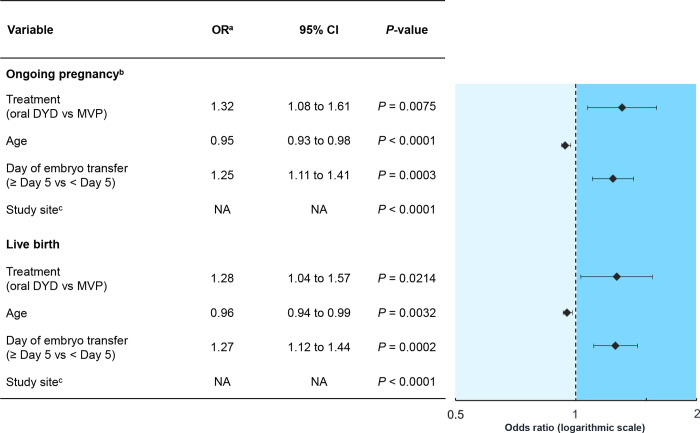
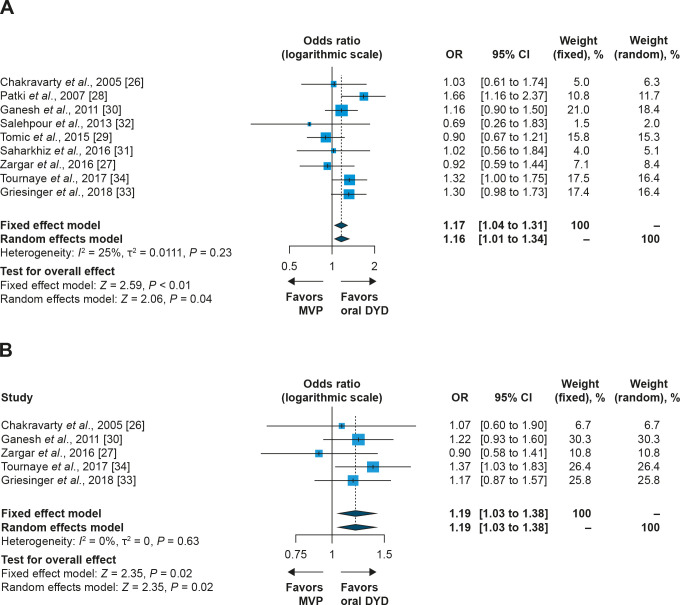
The aim of this systematic review and meta-analysis was to conduct a comprehensive assessment of the evidence on the efficacy and safety of oral dydrogesterone versus micronized vaginal progesterone (MVP) for luteal phase support. Embase and MEDLINE were searched for studies that evaluated the effect of luteal phase support with daily administration of oral dydrogesterone (20 to 40 mg) versus MVP capsules (600 to 800 mg) or gel (90 mg) on pregnancy or live birth rates in women undergoing fresh-cycle IVF (protocol registered at PROSPERO [CRD42018105949]). Individual participant data (IPD) were extracted for the primary analysis where available and aggregate data were extracted for the secondary analysis. Nine studies were eligible for inclusion; two studies had suitable IPD (full analysis sample: n = 1957). In the meta-analysis of IPD, oral dydrogesterone was associated with a significantly higher chance of ongoing pregnancy at 12 weeks of gestation (odds ratio [OR], 1.32; 95% confidence interval [CI], 1.08 to 1.61; P = 0.0075) and live birth (OR, 1.28; 95% CI, 1.04 to 1.57; P = 0.0214) compared to MVP. A meta-analysis combining IPD and aggregate data for all nine studies also demonstrated a statistically significant difference between oral dydrogesterone and MVP (pregnancy: OR, 1.16; 95% CI, 1.01 to 1.34; P = 0.04; live birth: OR, 1.19; 95% CI, 1.03 to 1.38; P = 0.02). Safety parameters were similar between the two groups. Collectively, this study indicates that a higher pregnancy rate and live birth rate may be obtained in women receiving oral dydrogesterone versus MVP for luteal phase support.
Conflict of interest statement
G.G.'s institution has received investigator fees from Abbott during the conduct of the Lotus I and Lotus II studies. Outside of this submitted work, G.G. has received nonfinancial support from MSD, Ferring, Merck Serono, IBSA, Finox, TEVA, Glycotope and Gedeon Richter, as well as personal fees from MSD, Ferring, Merck Serono, IBSA, Finox, TEVA, Glycotope, Vitrolife, NMC Healthcare, ReprodWissen, Biosilu, Gedeon Richter and ZIVA. C.B.’s institution has received investigator fees from Abbott during the conduct of the Lotus I and Lotus II studies. C.B. is the President of the Belgian Society of Reproductive Medicine (unpaid) and Section Editor of Reproductive BioMedicine Online. C.B. has received grants from Ferring, participated in an MSD-sponsored trial and has received consultancy fees from Ferring, MSD, BioMérieux, Abbott and Merck. E.K. is an employee of Abbott Laboratories GmbH, Hannover, Germany and owns shares of Abbott. C.P.-F. is an employee of Abbott GmbH & Co. KG, Wiesbaden, Germany and owns shares in Abbott. J.I.O. is an employee of Abbott Products Operations AG, Allschwil, Switzerland. S.D. is an employee of Abbott Healthcare Products BV, Weesp, The Netherlands and owns shares in Abbott. H.T.'s institution has received investigator fees from Abbott during the conduct of the Lotus I and Lotus II studies. H.T.’s institution has received grants from Merck, MSD, Goodlife, Cook, Roche, CooperSurgical, Besins, Ferring and Allergan. H.T. has received consultancy fees from Gedeon Richter, Merck, Ferring, Abbott and ObsEva. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Beckers NG, Macklon NS, Eijkemans MJ, Ludwig M, Felberbaum RE, Diedrich K, et al. Nonsupplemented luteal phase characteristics after the administration of recombinant human chorionic gonadotropin, recombinant luteinizing hormone, or gonadotropin-releasing hormone (GnRH) agonist to induce final oocyte maturation in in vitro fertilization patients after ovarian stimulation with recombinant follicle-stimulating hormone and GnRH antagonist cotreatment. J Clin Endocrinol Metab. 2003;88(9):4186–92. Epub 2003/09/13. 10.1210/jc.2002-021953 . - DOI - PubMed
-
- Kolibianakis EM, Bourgain C, Platteau P, Albano C, Van Steirteghem AC, Devroey P. Abnormal endometrial development occurs during the luteal phase of nonsupplemented donor cycles treated with recombinant follicle-stimulating hormone and gonadotropin-releasing hormone antagonists. Fertil Steril. 2003;80(2):464–6. Epub 2003/08/12. 10.1016/s0015-0282(03)00663-0 . - DOI - PubMed
-
- Macklon NS, Fauser BC. Impact of ovarian hyperstimulation on the luteal phase. J Reprod Fertil Suppl. 2000;55:101–8. Epub 2000/07/13. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
