

Assessment of Dietary Sodium Intake Using the Scored Salt Questionnaire in Autosomal Dominant Polycystic Kidney Disease
- PMID: 33147804
- PMCID: PMC7692491
- DOI: 10.3390/nu12113376
Assessment of Dietary Sodium Intake Using the Scored Salt Questionnaire in Autosomal Dominant Polycystic Kidney Disease
Abstract
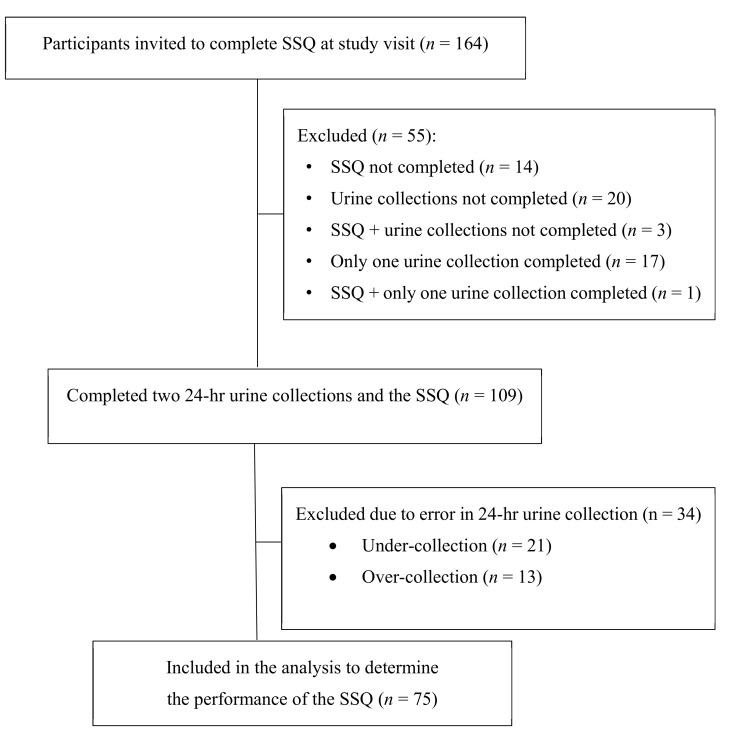
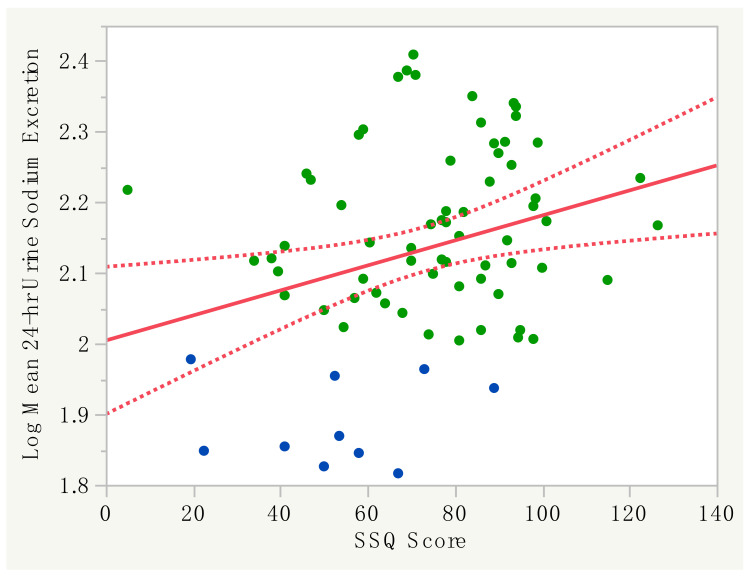
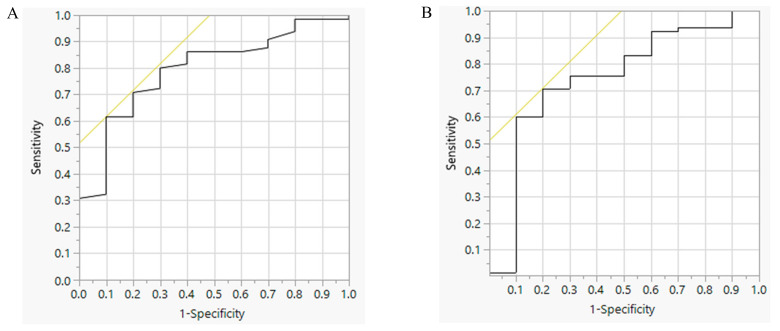
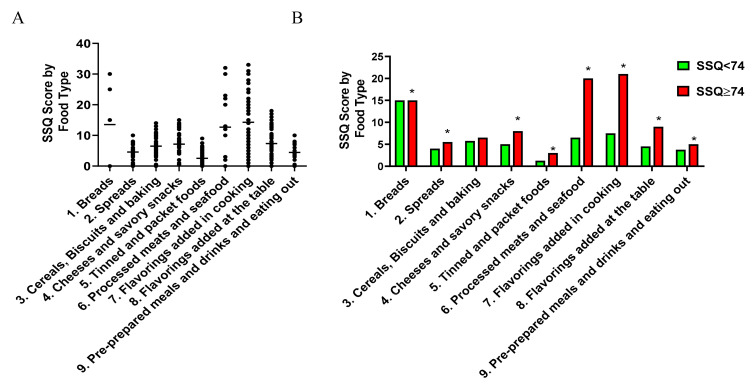
The excess intake of dietary sodium is a key modifiable factor for reducing disease progression in autosomal dominant polycystic kidney disease (ADPKD). The aim of this study was to test the hypothesis that the scored salt questionnaire (SSQ; a frequency questionnaire of nine sodium-rich food types) is a valid instrument to identify high dietary salt intake in ADPKD. The performance of the SSQ was evaluated in adults with ADPKD with an estimated glomerular filtration rate (eGFR) ≥ 30 mL/min/1.73 m2 during the screening visit of the PREVENT-ADPKD trial. High dietary sodium intake (HSI) was defined by a mean 24-h urinary sodium excretion ≥ 100 mmol/day from two collections. The median 24-h urine sodium excretion was 132 mmol/day (IQR: 112-172 mmol/d) (n = 75; mean age: 44.6 ± 11.5 years old; 53% female), and HSI (86.7% of total) was associated with male gender and higher BMI and systolic blood pressure (p < 0.05). The SSQ score (73 ± 23; mean ± SD) was weakly correlated with log10 24-h urine sodium excretion (r = 0.29, p = 0.01). Receiving operating characteristic analysis showed that the optimal cut-off point in predicting HSI was an SSQ score of 74 (area under the curve 0.79; sensitivity 61.5%; specificity 90.0%; p < 0.01). The evaluation of the SSQ in participants with a BMI ≥ 25 (n = 46) improved the sensitivity (100%) and the specificity (100%). Consumers with an SSQ score ≥ 74 (n = 41) had higher relative percentage intake of processed meats/seafood and flavourings added to cooking (p < 0.05). In conclusion, the SSQ is a valid tool for identifying high dietary salt intake in ADPKD but its value proposition (over 24-h urinary sodium measurement) is that it may provide consumers and their healthcare providers with insight into the potential origin of sodium-rich food sources.
Keywords: 24-h urine; autosomal dominant polycystic kidney disease; diet; food frequency questionnaire; progression; salt; sodium.
Conflict of interest statement
G. Rangan receives research grant support from Danone Research, Otsuka Pharmaceuticals and has been a site investigator for clinical trials sponsored by Sanofi, Reata Pharmaceuticals. G. Rangan also receives grant support from NHMRC and PKD Australia. D. Johnson has received consultancy fees, research grants, speaker’s honoraria and travel sponsorships from Baxter Healthcare and Fresenius Medical Care, consultancy fees from Astra Zeneca and AWAK, speaker’s honoraria and travel sponsorships from ONO, and travel sponsorships from Amgen. He is a current recipient of an Australian National Health and Medical Research Council Practitioner Fellowship. The authors have no other relevant affiliations or financial involvement with any organisation or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures
References
-
- Torres V.E., Abebe K.Z., Schrier R.W., Perrone R.D., Chapman A.B., Yu A.S., Braun W.E., Steinman T.I., Brosnahan G., Hogan M.C., et al. Dietary salt restriction is beneficial to the management of autosomal dominant polycystic kidney disease. Kidney Int. 2017;91:493–500. doi: 10.1016/j.kint.2016.10.018. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
