

Economic Burden of Osteoporosis-Related Fractures in the US Medicare Population
- PMID: 33148010
- PMCID: PMC8135238
- DOI: 10.1177/1060028020970518
Economic Burden of Osteoporosis-Related Fractures in the US Medicare Population
Abstract
Background: Osteoporosis-related fractures are an important public health burden.
Objective: To examine health care costs in Medicare patients with an osteoporosis-related fracture.
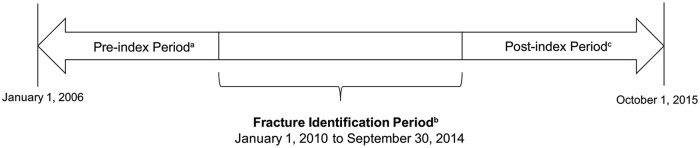
Methods: Medicare fee-for-service members with an osteoporosis-related fracture between January 1, 2010, to September 30, 2014 were included. A nonfracture comparator group was selected by propensity score matching. Generalized linear models using a gamma distribution were used to compare costs between fracture and nonfracture cohorts.
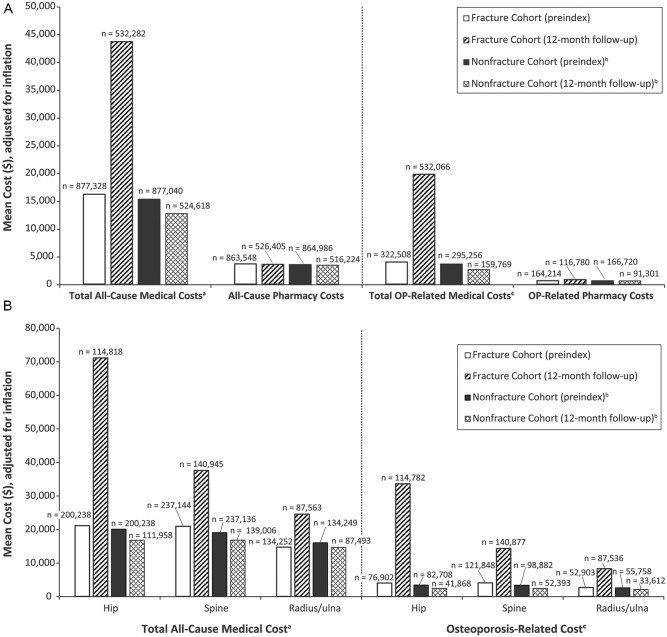
Results: A total of 885 676 Medicare beneficiaries had fracture(s) and met inclusion criteria. Average age was 80.5 (±8.4) years; 91% were White, and 94% female. Mean all-cause costs were greater in the fracture vs nonfracture cohort ($47 163.25 vs $16 034.61) overall and for men ($52 273.79 vs $17 352.68). The highest mean costs were for skilled nursing facility ($29 216), inpatient costs ($24 190.19), and hospice care ($20 996.83). The highest incremental costs versus the nonfracture cohort were for hip ($71 057.83 vs $16 807.74), spine ($37 543.87 vs $16 860.49), and radius/ulna ($24 505.27 vs $14 673.86). Total medical and pharmacy costs for patients who experienced a second fracture were higher compared with those who did not ($78 137.59 vs $44 467.47). Proportionally more patients in the fracture versus nonfracture cohort died (18% vs 9.3%), with higher death rates among men (20% vs 11%).
Conclusion and relevance: The current findings suggest a significant economic burden associated with fractures. Early identification and treatment of patients at high risk for fractures is of paramount importance for secondary prevention and reduced mortality.
Keywords: Medicare; cost; fracture; male; osteoporosis.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
