

Reprogramming the tumour microenvironment by radiotherapy: implications for radiotherapy and immunotherapy combinations
- PMID: 33148287
- PMCID: PMC7640712
- DOI: 10.1186/s13014-020-01678-1
Reprogramming the tumour microenvironment by radiotherapy: implications for radiotherapy and immunotherapy combinations
Abstract
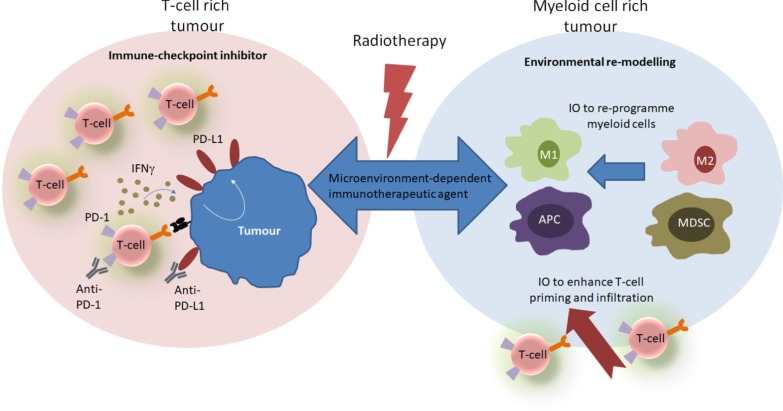
Radiotherapy (RT) is a highly effective anti-cancer therapy delivered to around 50-60% of patients. It is part of therapy for around 40% of cancer patients who are cured of their disease. Until recently, the focus of this anti-tumour efficacy has been on the direct tumour cytotoxicity and RT-induced DNA damage. Recently, the immunomodulatory effects of RT on the tumour microenvironment have increasingly been recognized. There is now intense interest in potentially using RT to induce an anti-tumour immune response, which has led to rethinking into how the efficacy of RT could be further enhanced. Following the breakthrough of immune check point inhibitors (ICIs), a new era of immuno-oncology (IO) agents has emerged and established immunotherapy as a routine part of cancer treatment. Despite ICI improving outcomes in many cancer types, overall durable responses occur in only a minority of patients. The immunostimulatory effects of RT make combinations with ICI attractive to potentially amplify anti-tumour immunity resulting in increased tumour responses and improved outcomes. In contrast, tumours with profoundly immunosuppressive tumour microenvironments, dominated by myeloid-derived cell populations, remain a greater clinical challenge and RT may potentially further enhance the immunosuppression. To harness the full potential of RT and IO agent combinations, further insights are required to enhance our understanding of the role these immunosuppressive myeloid populations play, how RT influences these populations and how they may be therapeutically manipulated in combination with RT to improve outcomes further. These are exciting times with increasing numbers of IO targets being discovered and IO agents undergoing clinical evaluation. Multidisciplinary research collaborations will be required to establish the optimal parameters for delivering RT (target volume, dose and fractionation) in combination with IO agents, including scheduling to achieve maximal therapeutic efficacy.
Keywords: Immune checkpoints; Immuno-oncology agents; Immunotherapy; Radiation therapy; Radiotherapy.
Conflict of interest statement
The authors declares that they have no competing interests.
Figures

References
-
- Balar AV, Galsky MD, Rosenberg JE, Powles T, Petrylak DP, Bellmunt J, et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial. Lancet. 2017;389(10064):67–76. doi: 10.1016/S0140-6736(16)32455-2. - DOI - PMC - PubMed
-
- Fehrenbacher L, Spira A, Ballinger M, Kowanetz M, Vansteenkiste J, Mazieres J, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet. 2016;387(10030):1837–1846. doi: 10.1016/S0140-6736(16)00587-0. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
