

Update of takotsubo syndrome in the era of COVID-19
- PMID: 33148469
- PMCID: PMC7556854
- DOI: 10.1016/j.jjcc.2020.10.004
Update of takotsubo syndrome in the era of COVID-19
Abstract
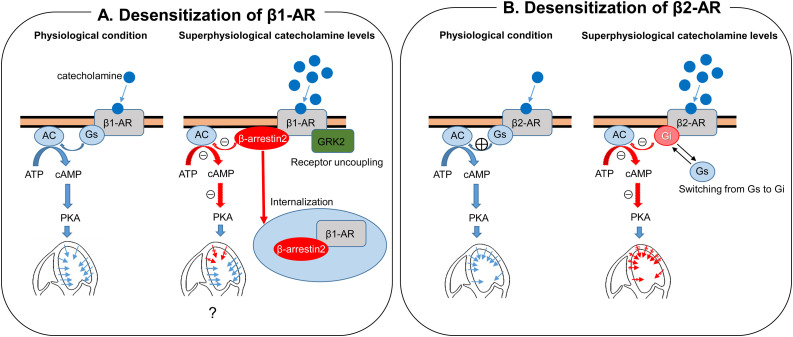
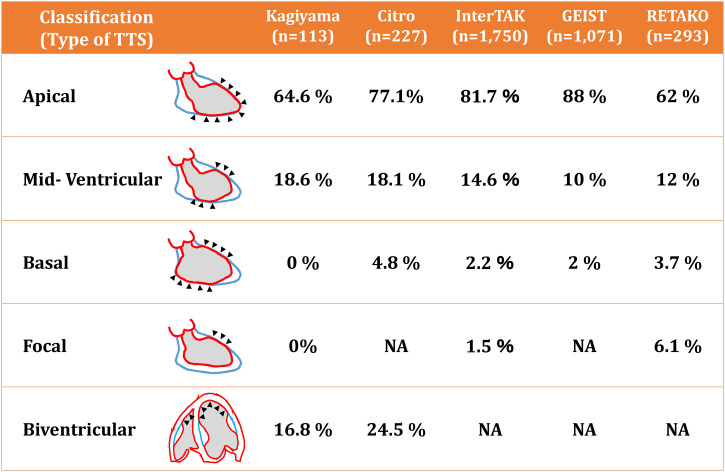
Takotsubo cardiomyopathy or takotsubo syndrome (TTS) has become a well-known disease not only in Japan but also in the rest of the world. Early reports suggested that TTS is a self-limiting disease with better prognosis than acute coronary syndrome. However, recent data showed that TTS is not a benign disease as compared with acute coronary syndrome. In addition to the apical ballooning, several other types of wall motion abnormalities have been classified as variants of TTS. In particular, right ventricular involvement, or biventricular TTS, is not uncommon and is associated with poor in-hospital as well as long-term outcomes. With respect to the pathophysiology, modulation (desensitization) of the beta-adrenergic receptor is suspected as a possible mechanism for transiently depressed myocardial contraction. Although specific treatments to improve prognosis of TTS are still uncertain, observational data suggest favorable impact of angiotensin-converting enzyme inhibitors or angiotensin receptor blockers. Finally, in the era of COVID-19, we should pay attention to a variety of cardiovascular conditions related to COVID-19. TTS is one of these conditions that can be triggered by both emotional and physical impact of the COVID-19 pandemic.
Keywords: COVID-19; Echocardiography; Takotsubo syndrome.
Copyright © 2020 Japanese College of Cardiology. Published by Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Is modulation (desensitization) of the beta-adrenergic receptors a cause or an epiphenomenon of takotsubo syndrome?J Cardiol. 2021 May;77(5):552. doi: 10.1016/j.jjcc.2021.01.008. Epub 2021 Feb 19. J Cardiol. 2021. PMID: 33618974 Free PMC article. No abstract available.
References
-
- Iga K., Gen H., Tomonaga G., Matsumura T., Hori K. Reversible left ventricular wall motion impairment caused by pheochromocytoma--a case report. Jpn Circ J. 1989;53:813–818. - PubMed
-
- Iga K., Hori K. Rapidly progressive deteriorated left ventricular wall motion associated with tetanus: a case report. Jpn J Med. 1990;29:305–308. - PubMed
-
- Dote K., Sato H., Tateishi H., Uchida T., Ishihara M. [Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases] J Cardiol. 1991;21:203–214. - PubMed
-
- Iga K., Hori K., Kitaguchi K., Matsumura T., Gen H., Tomonaga G. Transient segmental asynergy of the left ventricle of patients with various clinical manifestations possibly unrelated to the coronary artery disease. Jpn Circ J. 1991;55:1061–1067. - PubMed
-
- Tsuchihashi K., Ueshima K., Uchida T., Oh-mura N., Kimura K., Owa M. Transient left ventricular apical ballooning without coronary artery stenosis: a novel heart syndrome mimicking acute myocardial infarction. Angina Pectoris-Myocardial Infarction Investigations in Japan. J Am Coll Cardiol. 2001;38:11–18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
