

Pre-clinical tumor models of primary brain tumors: Challenges and opportunities
- PMID: 33148506
- PMCID: PMC7856042
- DOI: 10.1016/j.bbcan.2020.188458
Pre-clinical tumor models of primary brain tumors: Challenges and opportunities
Abstract
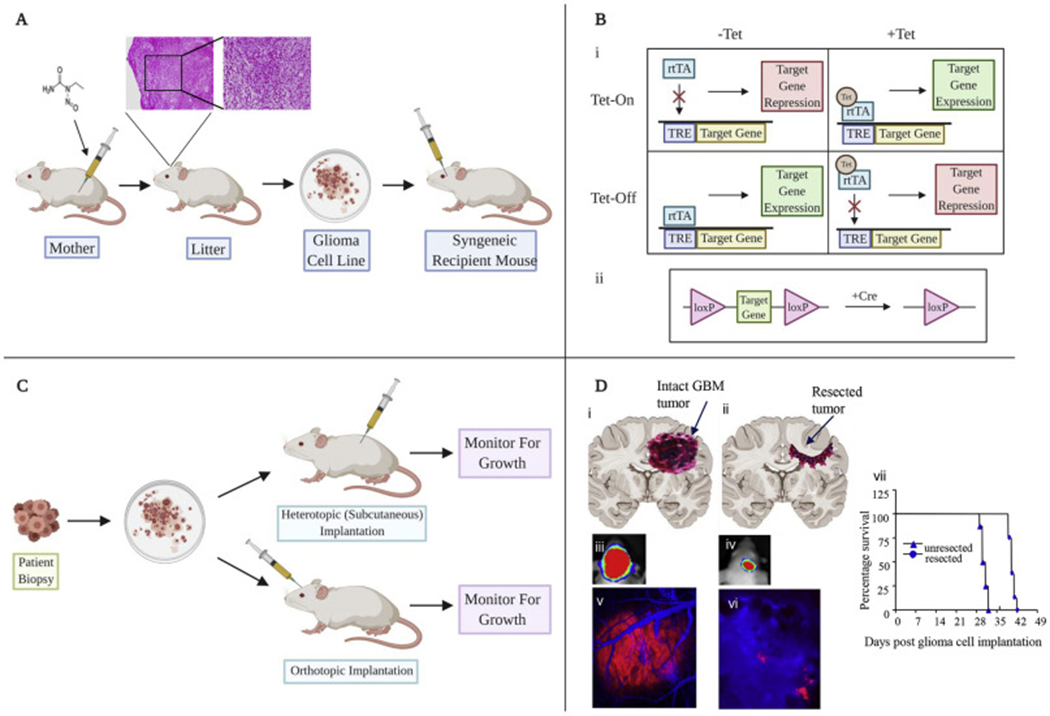
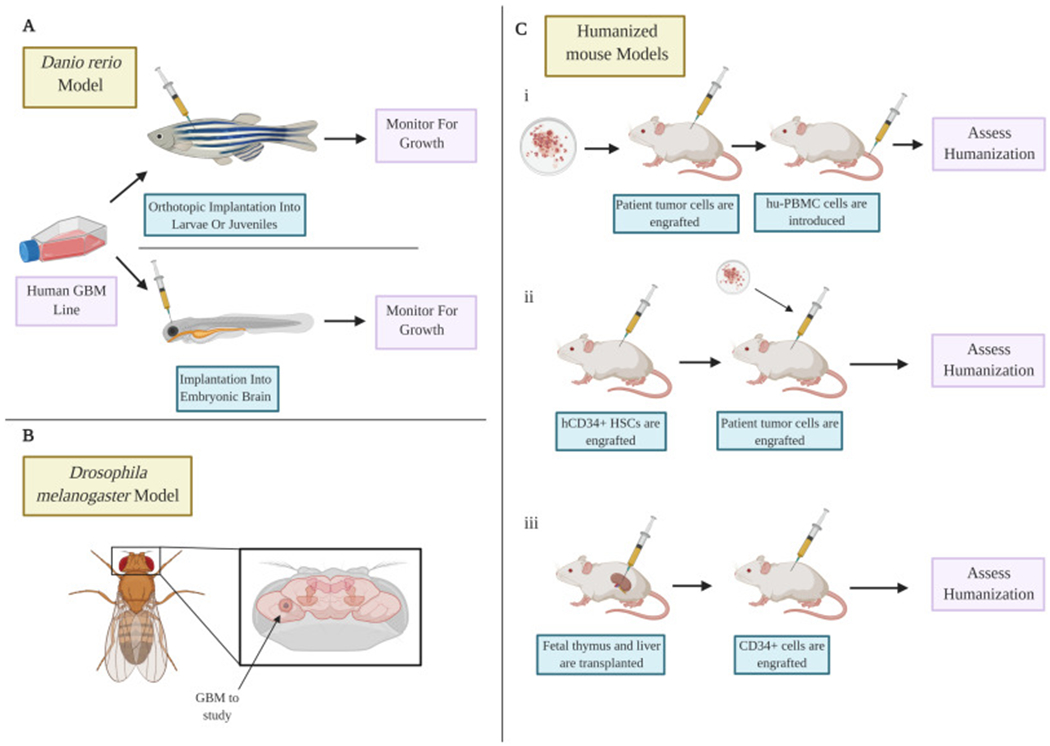
Primary brain tumors are a heterogeneous group of malignancies that originate in cells of the central nervous system. A variety of models tractable for preclinical studies have been developed to recapitulate human brain tumors, allowing us to understand the underlying pathobiology and explore potential treatments. However, many promising therapeutic strategies identified using preclinical models have shown limited efficacy or failed at the clinical trial stage. The inability to develop therapeutic strategies that significantly improve survival rates in patients highlight the compelling need to revisit the design of currently available animal models and explore the use of new models that allow us to bridge the gap between promising preclinical findings and clinical translation. In this review, we discuss current strategies used to model glioblastoma, the most malignant brain tumor in adults and highlight the shortcomings of specific models that must be circumvented for the development of innovative therapeutic strategies.
Keywords: Brain tumor model; Glioblastoma; Glioma; Neurooncology; Therapeutic development.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflict of interests
K.S. owns equity in and is a member of the Board of Directors of AMASA Therapeutics, a company developing stem cell-based therapies for cancer. K.S.’s interests were reviewed and are managed by Brigham and Women’s Hospital and Partners Healthcare in accordance with their conflict of interest policies. The other authors declare that they have no competing interests.
Figures
References
-
- Perkins A & Liu G (2016) Primary Brain Tumors in Adults: Diagnosis and Treatment. Am Fam Physician 93(3):211–217. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
