

Mortality due to cancer treatment delay: systematic review and meta-analysis
- PMID: 33148535
- PMCID: PMC7610021
- DOI: 10.1136/bmj.m4087
Mortality due to cancer treatment delay: systematic review and meta-analysis
Abstract
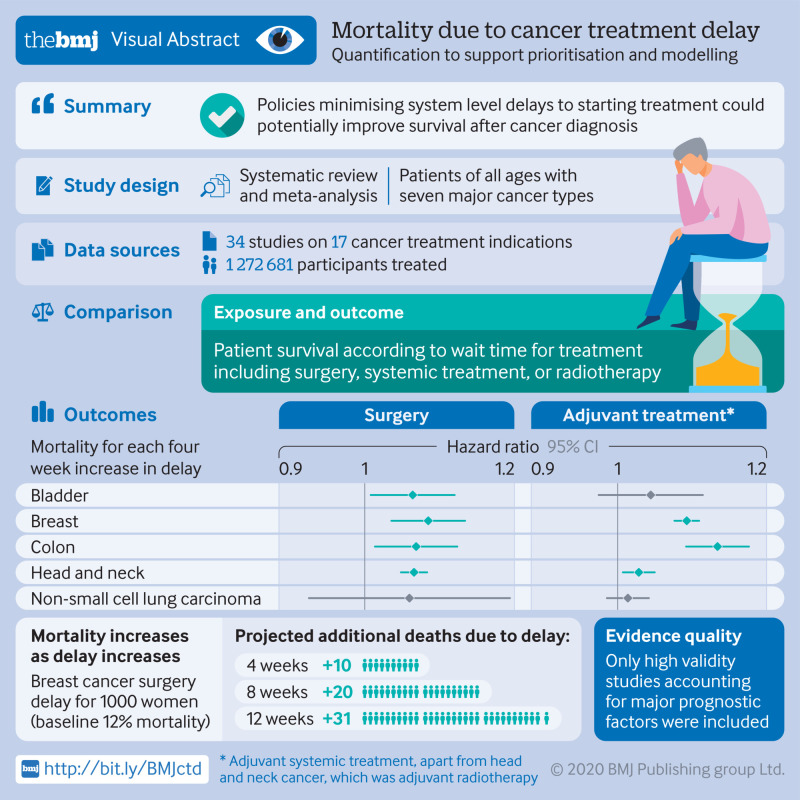
Objective: To quantify the association of cancer treatment delay and mortality for each four week increase in delay to inform cancer treatment pathways.
Design: Systematic review and meta-analysis.
Data sources: Published studies in Medline from 1 January 2000 to 10 April 2020.
Eligibility criteria for selecting studies: Curative, neoadjuvant, and adjuvant indications for surgery, systemic treatment, or radiotherapy for cancers of the bladder, breast, colon, rectum, lung, cervix, and head and neck were included. The main outcome measure was the hazard ratio for overall survival for each four week delay for each indication. Delay was measured from diagnosis to first treatment, or from the completion of one treatment to the start of the next. The primary analysis only included high validity studies controlling for major prognostic factors. Hazard ratios were assumed to be log linear in relation to overall survival and were converted to an effect for each four week delay. Pooled effects were estimated using DerSimonian and Laird random effect models.
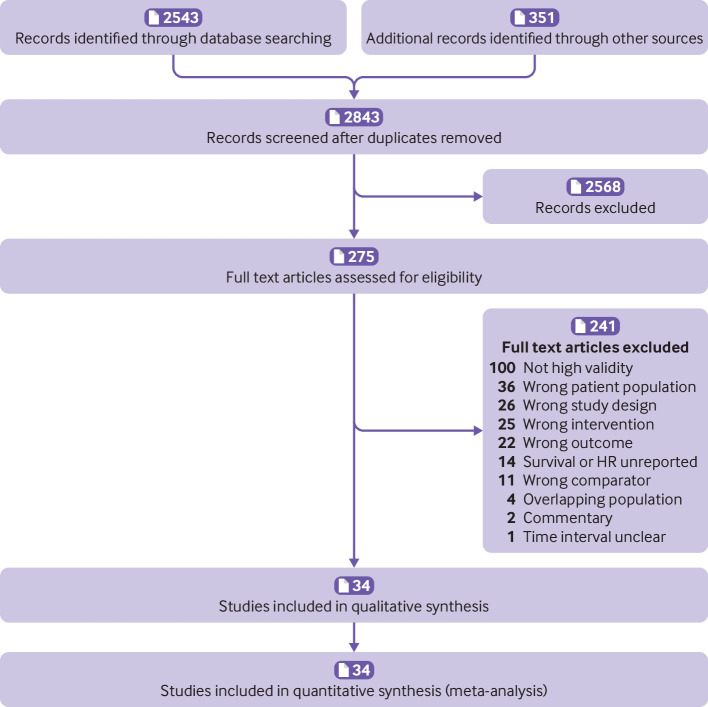
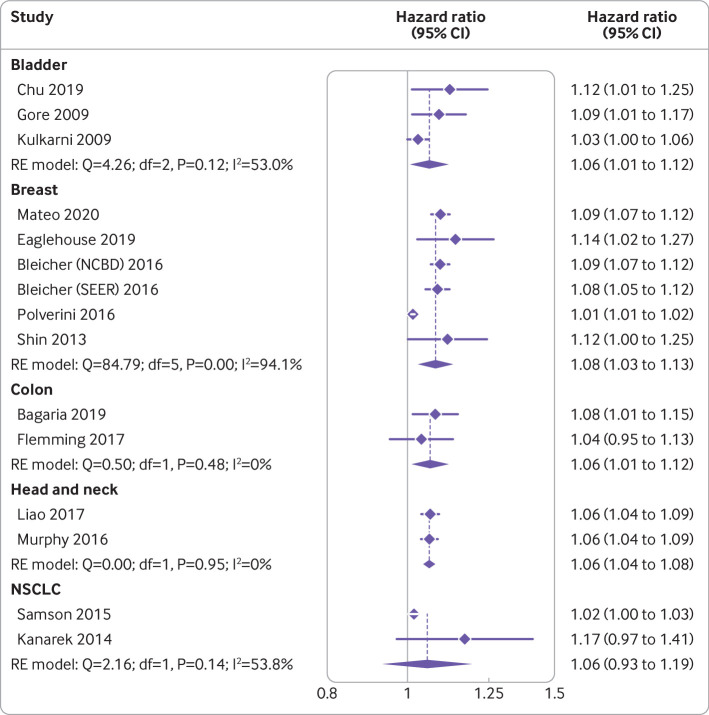
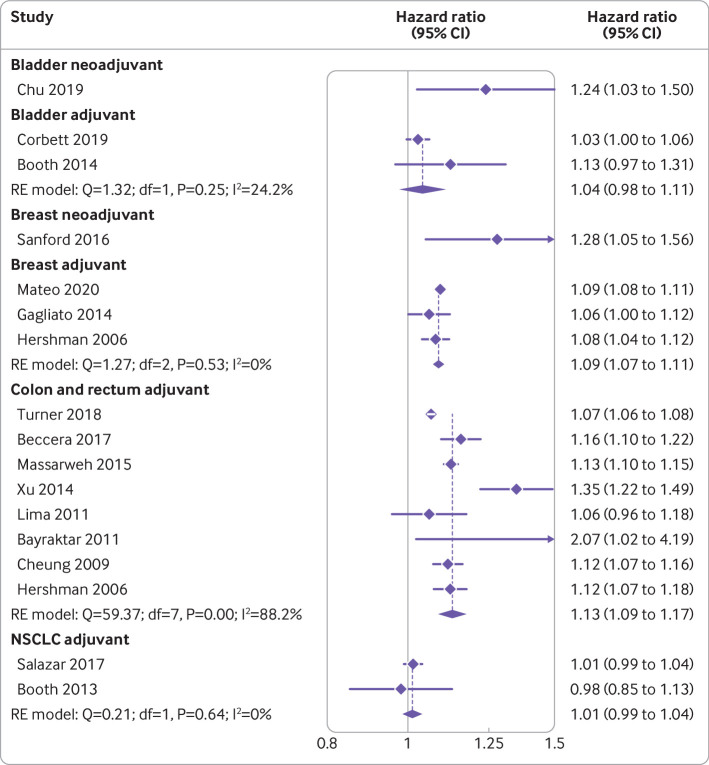
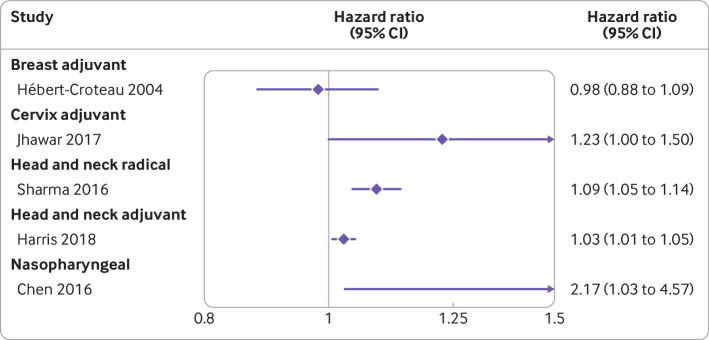
Results: The review included 34 studies for 17 indications (n=1 272 681 patients). No high validity data were found for five of the radiotherapy indications or for cervical cancer surgery. The association between delay and increased mortality was significant (P<0.05) for 13 of 17 indications. Surgery findings were consistent, with a mortality risk for each four week delay of 1.06-1.08 (eg, colectomy 1.06, 95% confidence interval 1.01 to 1.12; breast surgery 1.08, 1.03 to 1.13). Estimates for systemic treatment varied (hazard ratio range 1.01-1.28). Radiotherapy estimates were for radical radiotherapy for head and neck cancer (hazard ratio 1.09, 95% confidence interval 1.05 to 1.14), adjuvant radiotherapy after breast conserving surgery (0.98, 0.88 to 1.09), and cervix cancer adjuvant radiotherapy (1.23, 1.00 to 1.50). A sensitivity analysis of studies that had been excluded because of lack of information on comorbidities or functional status did not change the findings.
Conclusions: Cancer treatment delay is a problem in health systems worldwide. The impact of delay on mortality can now be quantified for prioritisation and modelling. Even a four week delay of cancer treatment is associated with increased mortality across surgical, systemic treatment, and radiotherapy indications for seven cancers. Policies focused on minimising system level delays to cancer treatment initiation could improve population level survival outcomes.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; unrestricted research funding for an unrelated project from Roche (TPH); no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Prioritising research into cancer treatment delays.BMJ. 2020 Nov 4;371:m4261. doi: 10.1136/bmj.m4261. BMJ. 2020. PMID: 33148613 No abstract available.
-
Delay in cancer treatment is associated with increased mortality.Evid Based Nurs. 2022 Jul;25(3):101. doi: 10.1136/ebnurs-2020-103390. Epub 2021 Sep 29. Evid Based Nurs. 2022. PMID: 34588300 No abstract available.
References
-
- Institute of Medicine Committee on Quality of Health Care in America Crossing the quality chasm: a new health system for the 21st century. National Academy Press, 2001.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous