

RECIST and iRECIST criteria for the evaluation of nivolumab plus ipilimumab in patients with microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: the GERCOR NIPICOL phase II study
- PMID: 33148693
- PMCID: PMC7640587
- DOI: 10.1136/jitc-2020-001499
RECIST and iRECIST criteria for the evaluation of nivolumab plus ipilimumab in patients with microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: the GERCOR NIPICOL phase II study
Abstract
Background: Immune checkpoint inhibitors (ICIs) are highly effective in patients with microsatellite instability/mismatch repair-deficient (MSI/dMMR) metastatic colorectal cancer (mCRC). Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 criteria may underestimate response to ICIs due to the pseudoprogression phenomenon. The GERCOR NIPICOL phase II study aimed to evaluate the frequency of pseudoprogressions in patients with MSI/dMMR mCRC treated with nivolumab and ipilimumab.
Methods: Patients with MSI/dMMR mCRC previously treated with fluoropyrimidines, oxaliplatin, and irinotecan with/without targeted therapies received nivolumab 3 mg/kg plus ipilimumab 1 mg/kg every 3 weeks for four cycles then nivolumab 3 mg/kg every 2 weeks until progression or a maximum of 20 cycles. Computed tomography scan tumor assessments were done every 6 weeks for 24 weeks and then every 12 weeks. The primary endpoint was disease control rate at 12 weeks according to RECIST 1.1 and iRECIST by central review.
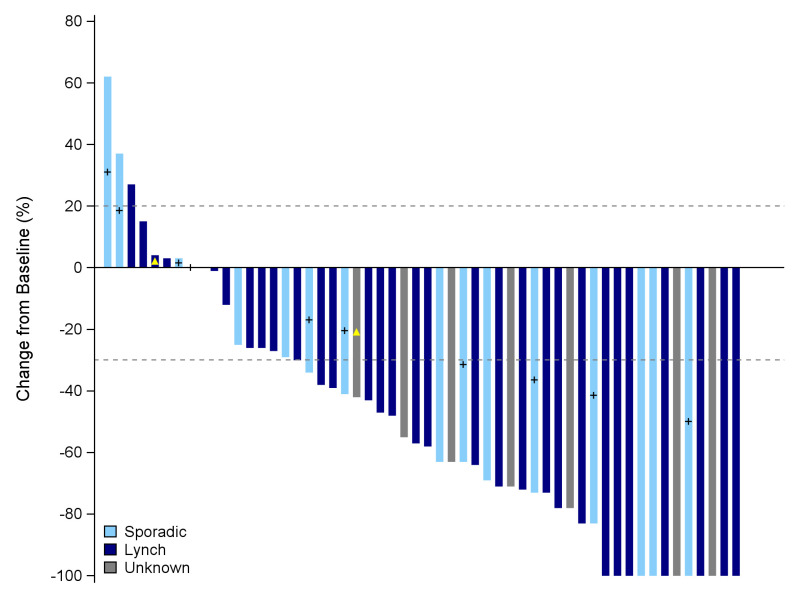
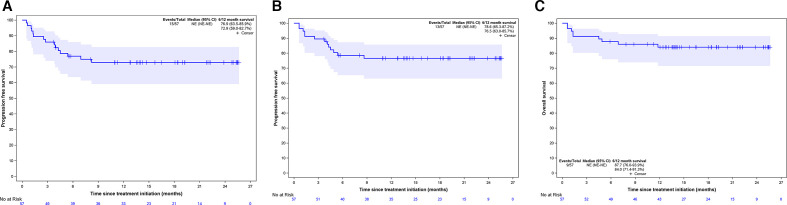
Results: Of 57 patients included between December 2017 and November 2018, 48.0% received ≥3 prior lines of chemotherapy, 18.0% had BRAFV600E mutation, and 56.0% had Lynch syndrome-related cancer. Seven patients (12.0%) discontinued treatment due to adverse events; one died due to a treatment-related adverse event. The disease control rate (DCR) at 12 weeks was 86.0% with RECIST 1.1% and 87.7% with iRECIST. Two pseudoprogressions (3.5%) were observed, at week 6 and at week 36, representing 18% of patients with disease progression per RECIST 1.1 criteria. With a median follow-up of 18.4 months, median progression-free survival (PFS) and overall survival (OS) were not reached. The 12-month PFS rate was 72.9% with RECIST 1.1% and 76.5% with iRECIST. The 12-month OS rate was 84%. Overall response rate was 59.7% with both criteria. RAS/BRAF status, sidedness, Lynch syndrome, and other baseline parameters were not associated with PFS.
Conclusion: Pseudoprogression is rare in patients with MSI/dMMR mCRC treated with nivolumab and ipilimumab. This combined ICI therapy confirms impressive DCR and survival outcomes in these patients.
Trial registration number: NCT03350126.
Keywords: CTLA-4 antigen; gastrointestinal neoplasms; immunotherapy; programmed cell death 1 receptor.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: TA reports consulting/advisory role and/or received honoraria from Amgen, Bristol-Myers Squibb, Chugai, Clovis, Gritstone Oncology, HalioDx, MSD Oncology, Pierre Fabre, Roche/Ventana, Sanofi, Servier, and Tesaro and has received travel, accommodations, and expenses from Roche/Genentech, MSD Oncology, and Bristol-Myers Squibb. JB reports consulting/advisory role and or received honoraria from Amgen, Bristol-Myers Squibb, MSD Oncology, Roche, Bayer, Servier, and AstraZeneca and has received travel and accommodations from Roche, MSD Oncology, and AstraZeneca. CB reports consulting/advisory role and/or received honoraria from Bayer, Sanofi, and Roche, and research grant from Roche. RC reports honoraria from Amgen, MSD Oncology, Sanofi, and Servier, and research grant from Servier Institute. TM reports honoraria from Amgen, Sanofi, Bristol-Myers Squibb, and Sandoz, travel, accommodations, or expenses by Amgen and research funding from Roche and Amgen. YM received honoraria from Bristol-Myers Squibb. MS reports consulting/advisory role and/or received honoraria from Bristol-Myers Squibb, Astellas, MSD Oncology, and Sanofi and has received travel, accommodations, and expenses from Bristol-Myers Squibb and Ventana/Roche. DT reports consulting/advisory role and/or received honoraria from Bristol-Myers Squibb, MSD Oncology, and Merck Serono and has received travel, accommodations, and expenses from MSD Oncology and Bristol-Myers Squibb.
Figures

References
-
- Llosa NJ, Cruise M, Tam A, et al. . The vigorous immune microenvironment of microsatellite instable colon cancer is balanced by multiple counter-inhibitory checkpoints. Cancer Discov 2015;5:43–51. 10.1158/2159-8290.CD-14-0863 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials