

CPAP management of COVID-19 respiratory failure: a first quantitative analysis from an inpatient service evaluation
- PMID: 33148777
- PMCID: PMC7643430
- DOI: 10.1136/bmjresp-2020-000692
CPAP management of COVID-19 respiratory failure: a first quantitative analysis from an inpatient service evaluation
Abstract
Objective: To evaluate the role of continuous positive air pressure (CPAP) in the management of respiratory failure associated with COVID-19 infection. Early clinical management with limited use of CPAP (3% of patients) was compared with a later clinical management strategy which had a higher proportion of CPAP use (15%).
Design: Retrospective case-controlled service evaluation for a single UK National Health Service (NHS) Trust during March-June 2020 designed and conducted solely to estimate the effects of current care.
Setting: The acute inpatient unit in Wrightington, Wigan and Leigh Teaching Hospitals NHS Foundation Trust, a medium-sized English NHS Trust.
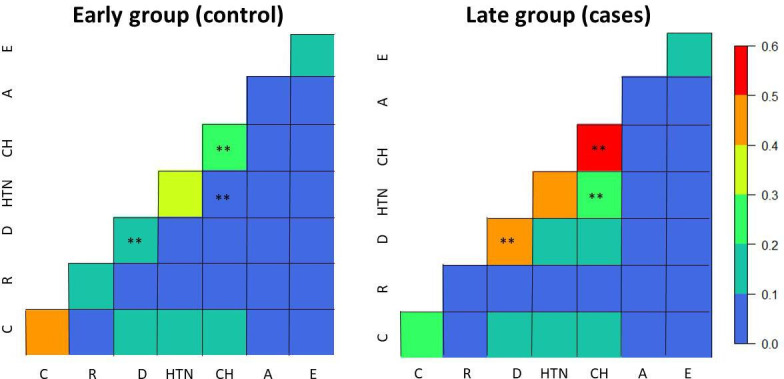
Participants: 206 patients with antigen confirmed COVID-19 disease and severe acute respiratory syndrome admitted between 17 March 2020 and 3 April 2020 for the early group (controls), and between 10 April 2020 and 11 May 2020 for the late group (cases). Follow-up for all cases was until 11 June by which time all patients had a final outcome of death or discharge. Both groups were composed of 103 patients. Cases and controls were matched by age and sex.
Outcome measure: The outcome measure was the proportion of patients surviving at time t (time from the positive result of COVID-19 test to discharge/death date). The predictors were CPAP intervention, intubation, residence in care homes and comorbidities (renal, pulmonary, cardiac, hypertension and diabetes). A stratified Cox proportional hazard for clustered data (via generalised estimating equations) and model selection algorithms were employed to identify the effect of CPAP on patients' survival and the effect on gas exchange as measured by alveolar arterial (A-a) gradient and timing of CPAP treatment on CPAP patients' survival.
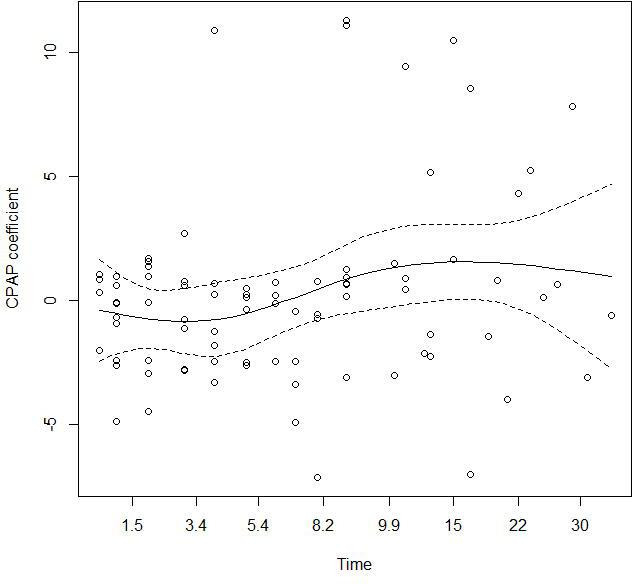
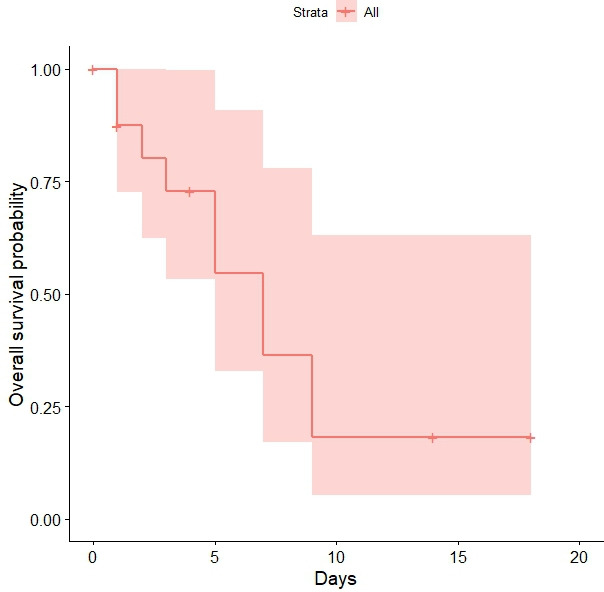
Results: CPAP was found to be significantly (HR 0.38, 95% CI 0.36 to 0.40) associated with lower risk of death in patients with hospital stay equal to, or below 7 days. However, for longer hospitalisation CPAP was found to be associated with increased risk of death (HR 1.72, 95% CI 1.40 to 2.12). When CPAP was initiated within 4 days of hospital admission, the survival probability was above 73% (95% CI 53% to 99%). In addition, lower A-a gradient was associated with lower risk of death in CPAP patients (HR 1.011, 95% CI 1.010 to 1.013). The selected model (best fit) was stratified by sex and clustered by case/control groups. The predictors were age, intubation, hypertension and the residency from care homes, which were found to be statistically significantly associated with patient's death/discharge.
Conclusions: CPAP is a simple and cost-effective intervention. It has been established for care of other respiratory disorders but not for COVID-19 respiratory failure. This evaluation establishes that CPAP as a potentially viable treatment option for this group of patients during the first days of hospital admission. As yet there is limited availability of quantitative research on CPAP use for COVID-19. Whist this work is hampered by both the relatively small sample size and retrospective design (which reduced the ability to control potential confounders), it represents evidence of the significant benefit of early CPAP intervention. This evaluation should stimulate further research questions and larger study designs on the potential benefit of CPAP for COVID-19 infections. Globally, this potentially beneficial low cost and low intensity therapy could have added significance economically for healthcare provision in less developed countries.
Keywords: ARDS; non invasive ventilation; pneumonia; respiratory infection; viral infection.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Bakke SA, Botker MT, Riddervold IS, et al. . Continuous positive airway pressure and noninvasive ventilation in prehospital treatment of patients with acute respiratory failure: a systematic review of controlled studies. Scand J Trauma Resusc Emerg Med 2014;22:69. 10.1186/s13049-014-0069-8 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous