

A Comparison of Patient-Reported Outcome Measures of Quality of Life By Dialysis Modality in the Treatment of Kidney Failure: A Systematic Review
- PMID: 33149924
- PMCID: PMC7580133
- DOI: 10.1177/2054358120957431
A Comparison of Patient-Reported Outcome Measures of Quality of Life By Dialysis Modality in the Treatment of Kidney Failure: A Systematic Review
Abstract
Background: There is an increasing demand to incorporate patient-reported outcome measures (PROMs) such as quality of life (QOL) in decision-making when selecting a chronic dialysis modality.
Objective: To compare the change in QOL over time among similar patients on different dialysis modalities to provide unique and novel insights on the impact of dialysis modality on PROMs.
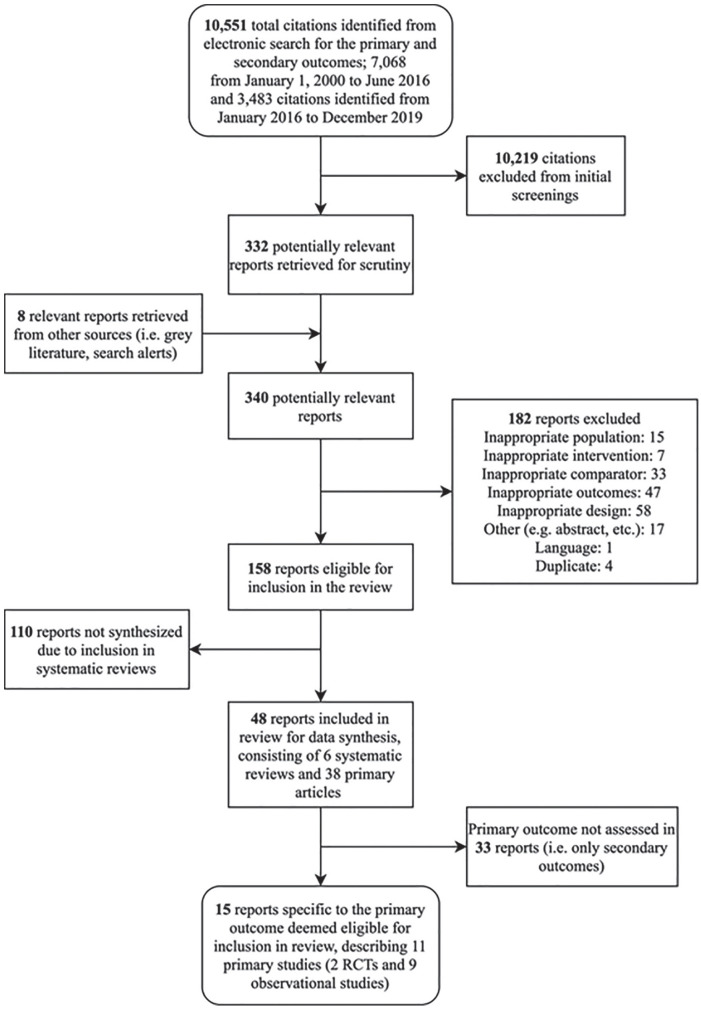
Design: Systematic reviews, randomized controlled trials, and nonrandomized controlled trials were examined via a comprehensive search strategy incorporating multiple bibliographic databases.
Setting: Data were extracted from relevant studies from January 1, 2000 to December 31, 2019 without limitations on country of study conduction.
Patients: Eligible studies included adults (≥18 years) with end-stage kidney disease of any cause who were prescribed dialysis treatment (either as lifetime treatment or bridge to transplant).
Measurements: The 5 comparisons were peritoneal dialysis (PD) vs in-center hemodialysis (ICHD), home hemodialysis (HHD) vs ICHD, HHD modalities compared with one another, HHD vs PD, and self-care ICHD vs traditional nurse-based ICHD.
Methods: Included studies compared adults on different dialysis modalities with repeat measures within individuals to determine changes in QOL between dialysis modalities (in-center or home dialysis). Methodological quality was assessed by the Scottish Intercollegiate Guidelines Network (SIGN 50) checklist. A narrative synthesis was conducted, synthesizing the direction and size of any observed effects across studies.
Results: Two randomized controlled trials and 9 prospective cohort studies involving a combined total of 3711 participants were included. Comparing PD and ICHD, 5 out of 9 studies found significant differences (P < .05) favoring PD in the change of multiple QOL domains, including "physical component score," "role of social component score," "cognitive status," "role limitation due to emotional function," "role limitation due to physical function," "bodily pain," "burden of kidney disease," "effects of kidney disease on daily life," "symptoms/problems," "sexual function," "finance," and "patient satisfaction." Conversely, 3 of these studies demonstrated statistically significant differences (P < .05) favoring ICHD in the domains of "role limitation due to physical function," "general health," "support from staff," "sleep quality," "social support," "health status," "social interaction," "body image," and "overall health." Comparing HHD and ICHD, significant differences (P < .05) favoring HHD for the QOL domains of "general health," "burden of kidney disease," and the visual analogue scale were reported.
Limitations: Our study is constrained by the small sample sizes of included studies, as well as heterogeneity among both study populations and validated QOL scales, limiting inter-study comparison.
Conclusions: We identified differences in specific QOL domains between dialysis modalities that may aid in patient decision-making based on individual priorities.
Trial registration: PROSPERO Registration Number: CRD42016046980.
Primary funding source: The original research for this study was derived from the Canadian Agency for Drugs and Technologies in Health (CADTH) 2017 optimal use report, titled "Dialysis Modalities for the Treatment of End-Stage Kidney Disease: A Health Technology Assessment." The CADTH receives funding from Canada's federal, provincial, and territorial governments, with the exception of Quebec.
Contexte: On observe une demande croissante pour intégrer des mesures des résultats déclarées par les patients (MRDP) comme la qualité de vie (QDV) dans la prise de décision quant à la modalité de dialyse.
Objectif: Comparer l’évolution de la QDV chez des patients de profils similaires, mais utilisant différentes modalités de dialyse, pour fournir un éclairage nouveau sur l’incidence de la modalité sur les MRDP.
Type d’étude: Des revues systématiques et des essais contrôlés avec ou sans répartition aléatoire ont été examinés dans le cadre d’une stratégie de recherche globale incorporant plusieurs bases de données bibliographiques.
Conception: Les données ont été extraites des études pertinentes entre le 1er janvier 2000 et le 31 décembre 2019 sans limitation relativement à l’origine (pays) de l’étude.
Sujets: Les études admissibles portaient sur des adultes atteints d’insuffisance rénale terminale (toutes causes) auxquels un traitement de dialyse avait été prescrit, soit comme traitement à vie, soit en attendant une transplantation.
Mesures: Ont été comparées 1) la dialyse péritonéale [DP] vs l’hémodialyse en centre [HDC]; 2) l’hémodialyse à domicile [HDD] vs l’HDC; 3) les modalités d’HDD les unes aux autres; 4) l’HDD vs la DP; et 5) l’HDC autogérée vs l’HDC traditionnelle sous supervision d’une infirmière.
Méthodologie: Les études incluses comparaient des adultes sous différentes modalités de dialyse et comportaient des mesures répétées permettant d’observer des changements dans la QDV selon la modalité (en centre ou à domicile). La qualité méthodologique a été évaluée avec la grille d’évaluation du Scottish Intercollegiate Guidelines Network (SIGN 50). Une synthèse narrative a été réalisée pour résumer la direction et l’ampleur de tous les effets observés dans les différentes études.
Résultats: Ont été inclus deux essais contrôlés à répartition aléatoire et neuf études de cohorte prospectives (3 711 patients au total). En comparant la DP à l’HDC, cinq des neufs études rapportaient des différences significatives (P<0,05) favorisant la DP dans plusieurs aspects de la QDV, notamment quant au « score de la composante physique », au « rôle du score de la composante sociale », à « l’état cognitif », à la « limitation dans les activités quotidiennes en raison des aspects émotionnels », à la « limitation dans les activités quotidiennes en raison des aspects physiques », à la « douleur physique », au « fardeau de la néphropathie », aux « conséquences de la néphropathie sur la QDV », aux « symptômes/problèmes », à la « fonction sexuelle », aux « conséquences financières » et à la « satisfaction du patient ». En revanche, trois de ces études montraient des différences statistiquement significatives (P<0,05) favorisant l’HDC dans les aspects suivants: « limitation dans les activités quotidiennes en raison des aspects physiques », « état de santé général », « soutien du personnel soignant », « qualité du sommeil », « soutien social », « état de santé », « interactions sociales », « image corporelle » et « état de santé global ». En comparant l’HDD et l’HDC, des différences significatives (P<0,05) favorisant l’HDD ont été rapportées en ce qui concerne « l’état de santé général », le « fardeau de la néphropathie » et l’échelle visuelle analogique.
Limites: L’étude est limitée par la faible taille des échantillons des études incluses, ainsi que par l’hétérogénéité des populations et des échelles validées pour la mesure de la QDV, ce qui restreint les comparaisons entre les études.
Conclusion: Des différences significatives touchant certains aspects propres à la qualité de vie ont été observées entre les différentes modalités de dialyse. Ces observations pourraient orienter une prise de décision en fonction des priorités individuelles des patients.
Keywords: dialysis; dialysis choice; health-related quality of life; peritoneal dialysis; quality of life.
© The Author(s) 2020.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.K. is the CMO—Quanta Dialysis Technologies.
Figures
Similar articles
-
Comparison of physical activity and quality of life in home haemodialysis (HHD) patients versus conventional in-centre haemodialysis (ICHD) patients: the observational, longitudinal, prospective, international, multicentric SeCoIA study protocol.BMC Nephrol. 2020 Nov 23;21(1):500. doi: 10.1186/s12882-020-02127-7. BMC Nephrol. 2020. PMID: 33225917 Free PMC article.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Burden of Kidney Disease, Health-Related Quality of Life, and Employment Among Patients Receiving Peritoneal Dialysis and In-Center Hemodialysis: Findings From the DOPPS Program.Am J Kidney Dis. 2021 Oct;78(4):489-500.e1. doi: 10.1053/j.ajkd.2021.02.327. Epub 2021 Apr 16. Am J Kidney Dis. 2021. PMID: 33872688
-
Choosing Home Hemodialysis: A Critical Review of Patient Outcomes.Blood Purif. 2018;45(1-3):224-229. doi: 10.1159/000485159. Epub 2018 Jan 26. Blood Purif. 2018. PMID: 29478056 Review.
-
Cost Controversies of a "Home Dialysis First" Policy.Can J Kidney Health Dis. 2019 Aug 30;6:2054358119871541. doi: 10.1177/2054358119871541. eCollection 2019. Can J Kidney Health Dis. 2019. PMID: 31516718 Free PMC article. Review.
Cited by
-
Body Composition Parameters Correlate to Depression Symptom Levels in Patients Treated with Hemodialysis and Peritoneal Dialysis.Int J Environ Res Public Health. 2023 Jan 27;20(3):2285. doi: 10.3390/ijerph20032285. Int J Environ Res Public Health. 2023. PMID: 36767652 Free PMC article.
-
Automated Peritoneal Dialysis: Patient Perspectives and Outcomes.Int J Nephrol Renovasc Dis. 2021 Oct 7;14:385-392. doi: 10.2147/IJNRD.S236553. eCollection 2021. Int J Nephrol Renovasc Dis. 2021. PMID: 34675604 Free PMC article. Review.
-
Multifaceted Sexual Dysfunction in Dialyzing Men and Women: Pathophysiology, Diagnostics, and Therapeutics.Life (Basel). 2021 Apr 2;11(4):311. doi: 10.3390/life11040311. Life (Basel). 2021. PMID: 33918412 Free PMC article. Review.
-
Returning to PD after kidney transplant failure is a valuable option.Int Urol Nephrol. 2022 May;54(5):1123-1126. doi: 10.1007/s11255-021-02980-x. Epub 2021 Sep 6. Int Urol Nephrol. 2022. PMID: 34487296
-
Quality of life trajectories for different dialysis modalities-a nationwide study.Clin Kidney J. 2024 Dec 20;18(2):sfae420. doi: 10.1093/ckj/sfae420. eCollection 2025 Feb. Clin Kidney J. 2024. PMID: 39968507 Free PMC article.
References
-
- Couchoud C, Bolignano D, Nistor I, et al. Dialysis modality choice in diabetic patients with end-stage kidney disease: a systematic review of the available evidence. Nephrol Dial Transplant. 2015;30(2):310-320. - PubMed
-
- Pike E, Hamidi V, Ringerike T, et al. Health technology assessment of the different dialysis modalities in Norway. Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH), NIPH Systematic Reviews, The Norwegian Institute of Public Health (NIPH); 2013. - PubMed
-
- Jiwakanon S, Chiu YW, Kalantar-Zadeh K, Mehrotra R. Peritoneal dialysis: an underutilized modality. Curr Opin Nephrol Hypertens. 2010;19(6):573-577. - PubMed
-
- Harwood L, Clark AM. Understanding pre-dialysis modality decision-making: a meta-synthesis of qualitative studies. Int J Nurs Stud. 2013;50(1):109-120. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
