

An Open-Label Prospective Study to Compare the Efficacy and Safety of Topical Fluticasone Versus Tacrolimus in the Proactive Treatment of Atopic Dermatitis
- PMID: 33150035
- PMCID: PMC7588157
- DOI: 10.5826/dpc.1004a94
An Open-Label Prospective Study to Compare the Efficacy and Safety of Topical Fluticasone Versus Tacrolimus in the Proactive Treatment of Atopic Dermatitis
Abstract
Background: Atopic dermatitis (AD), a chronic, recurrent inflammatory skin condition primarily affects children. Topical treatment, systemic treatment, and phototherapy are mainstays of treatment. Topical corticosteroids (TCS) are first-line therapy for AD but are associated with various adverse effects. Topical calcineurin inhibitors (TCI) can be used as an alternative to TCS.
Objective: The aim of the study is to compare the efficacy of topical preparations of fluticasone and tacrolimus in reducing the severity of disease and, to assess the quality of life (QoL), and to estimate if any association exists between severity of disease and QoL.
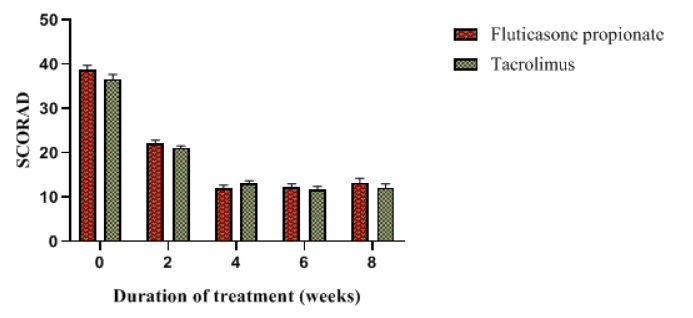
Methods: Thirty-seven children with AD randomly received one of the 2 topical treatments, with daily application for the first 4 weeks in the acute phase and twice weekly for next 4 weeks in the maintenance phase. The severity of disease was assessed using SCORing Atopic Dermatitis (SCORAD), and QoL was assessed using the Children's Dermatology Life Quality Index (CDLQI).
Results: At the end of the acute phase, there was a reduction in SCORAD score of 69.29% in the fluticasone group and 64.2% in the tacrolimus group (P < 0.001). In the maintenance phase, the score had risen in the fluticasone group by a mean difference of 0.81, while in the tacrolimus group it decreased by 0.99. Both fluticasone and tacrolimus groups improved in children's QoL (P < 0.001). Positive correlation (r = 0.4668) exists between SCORAD and QoL. The most common adverse skin reaction noted was skin burning with tacrolimus.
Conclusions: Fluticasone and tacrolimus are equally efficacious in the treatment of AD and have similar benefits with children's QoL. Tacrolimus is better than fluticasone at reducing the extent of lesions.
Keywords: atopic dermatitis; fluticasone propionate; tacrolimus; topical calcineurin inhibitors; topical corticosteroids.
©2020 Mudaliyar et al.
Conflict of interest statement
Competing interests: The authors have no conflicts of interest to disclose.
Figures




References
LinkOut - more resources
Full Text Sources