

Sodium glucose cotransporter 2 inhibitors: mechanisms of action in heart failure
- PMID: 33150520
- PMCID: PMC8024236
- DOI: 10.1007/s10741-020-10041-1
Sodium glucose cotransporter 2 inhibitors: mechanisms of action in heart failure
Abstract
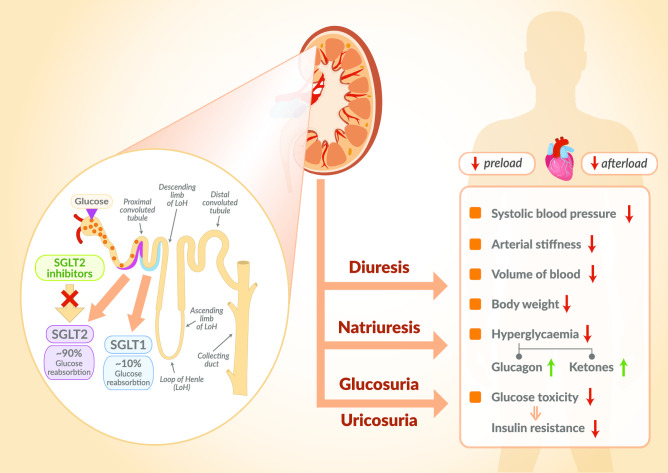
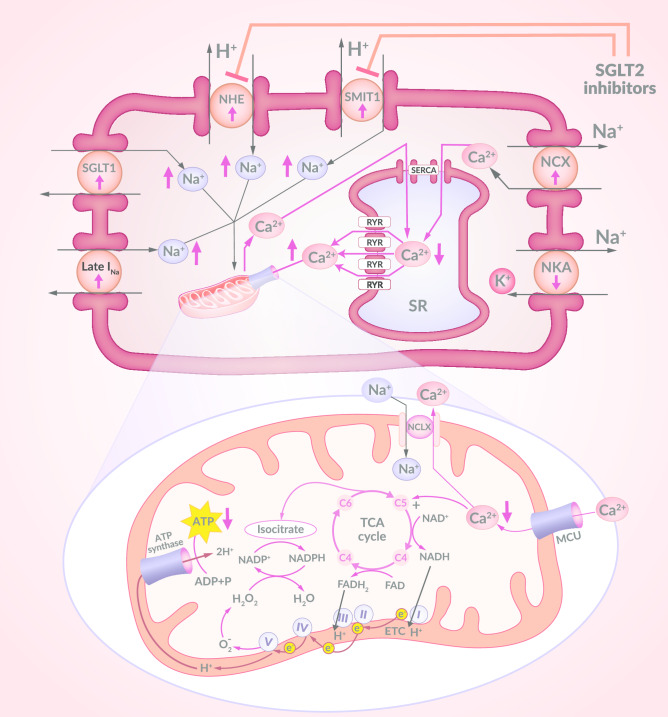
Diabetes is a key independent risk factor in the development of heart failure (HF) and a strong, adverse prognostic factor in HF patients. HF remains the primary cause of hospitalisation for diabetics and, as previous studies have shown, when HF occurs in these patients, intensive glycaemic control does not directly improve the prognosis. Recent clinical studies assessing a new class of antidiabetic drugs, sodium-glucose cotransporter 2 inhibitors (SGLT2is) showed some unexpected beneficial results. Patients treated with SGLT2is had a significant decrease in both cardiovascular (CV) and all-cause mortality and less hospitalisations due to HF compared to those given a placebo. These significant clinical benefits occurred quickly after the drugs were administered and were not solely due to improved glycaemic control. These groundbreaking clinical trials' results have already changed clinical practice in the management of patients with diabetes at high CV risk. These trials have triggered numerous experimental studies aimed at explaining the mechanisms of action of this unique group of drugs. This article presents the current state of knowledge about the mechanisms of action of SGLT2is developed for the treatment of diabetes and which, thanks to their cardioprotective effects, may, in the future, become a treatment for patients with HF.
Keywords: Cardiovascular diseases; Diabetes; Heart failure; Sodium-glucose cotransporter 2 inhibitors.
Conflict of interest statement
Mieczysław Dutka, Rafał Bobiński, Izabela Ulman-Włodarz, Maciej Hajduga, Jan Bujok, Celina Pająk,Michał Ćwiertnia have no conflicts of interest or financial ties to disclose.
Figures
Similar articles
-
Clinical Considerations for Use of SGLT2 Inhibitor Therapy in Patients with Heart Failure and Reduced Ejection Fraction: A Review.Adv Ther. 2022 Aug;39(8):3472-3487. doi: 10.1007/s12325-022-02169-3. Epub 2022 Jun 14. Adv Ther. 2022. PMID: 35699903 Free PMC article. Review.
-
Hypoglycemic Drugs in Patients with Diabetes Mellitus and Heart Failure: A Narrative Review.Medicina (Kaunas). 2024 May 30;60(6):912. doi: 10.3390/medicina60060912. Medicina (Kaunas). 2024. PMID: 38929529 Free PMC article. Review.
-
Lower risk of hospitalization for heart failure, kidney disease and death with sodium-glucose co-transporter-2 inhibitors compared with dipeptidyl peptidase-4 inhibitors in type 2 diabetes regardless of prior cardiovascular or kidney disease: A retrospective cohort study in UK primary care.Diabetes Obes Metab. 2021 Oct;23(10):2207-2214. doi: 10.1111/dom.14437. Epub 2021 Aug 2. Diabetes Obes Metab. 2021. PMID: 33973690 Free PMC article.
-
Sodium-glucose cotransporter 2 inhibitors: A comprehensive review from cells to bedside.Fundam Clin Pharmacol. 2023 Jun;37(3):481-492. doi: 10.1111/fcp.12852. Epub 2022 Dec 27. Fundam Clin Pharmacol. 2023. PMID: 36399066 Review.
-
Effects of sodium glucose cotransporter type 2 inhibitors on heart failure.Diabetes Obes Metab. 2019 Apr;21 Suppl 2:19-23. doi: 10.1111/dom.13678. Diabetes Obes Metab. 2019. PMID: 31081589 Review.
Cited by
-
Impact of Sacubitril/Valsartan on Circulating microRNA in Patients with Heart Failure.Biomedicines. 2023 Mar 28;11(4):1037. doi: 10.3390/biomedicines11041037. Biomedicines. 2023. PMID: 37189655 Free PMC article.
-
Impact of baseline left ventricular ejection fraction and body mass index on the effect of 24-week Ipragliflozin treatment on left ventricular diastolic function in patients with type 2 diabetes and chronic kidney disease: insights from the PROCEED trial.Cardiovasc Diabetol. 2025 May 2;24(1):190. doi: 10.1186/s12933-025-02745-1. Cardiovasc Diabetol. 2025. PMID: 40317024 Free PMC article. Clinical Trial.
-
Effect of Sodium-Glucose Co-transporter Protein 2 Inhibitors on Arrhythmia in Heart Failure Patients With or Without Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials.Front Cardiovasc Med. 2022 May 18;9:902923. doi: 10.3389/fcvm.2022.902923. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35665272 Free PMC article.
-
SGLT2 Inhibitors: The First Endothelial-Protector for Diabetic Nephropathy.J Clin Med. 2025 Feb 13;14(4):1241. doi: 10.3390/jcm14041241. J Clin Med. 2025. PMID: 40004772 Free PMC article. Review.
-
SGLT-2 Inhibitors in Cancer Treatment-Mechanisms of Action and Emerging New Perspectives.Cancers (Basel). 2022 Nov 25;14(23):5811. doi: 10.3390/cancers14235811. Cancers (Basel). 2022. PMID: 36497303 Free PMC article. Review.
References
-
- Neal B, Perkovic V, de Zeeuw D, Fulcher G, Erondu N, et al. Canagliflozin for primary and secondary prevention of cardiovascular events results from the CANVAS program (Canagliflozin Cardiovascular Assessment Study) Circulation. 2018;137:323–334. doi: 10.1161/CIRCULATIONAHA.117.032038. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
