

Hyperoxemia and Cerebral Vasospasm in Aneurysmal Subarachnoid Hemorrhage
- PMID: 33150573
- PMCID: PMC8093321
- DOI: 10.1007/s12028-020-01136-6
Hyperoxemia and Cerebral Vasospasm in Aneurysmal Subarachnoid Hemorrhage
Abstract
Background: Cerebral vasospasm is a major contributor to disability and mortality after aneurysmal subarachnoid hemorrhage. Oxidation of cell-free hemoglobin plays an integral role in neuroinflammation and is a suggested source of tissue injury after aneurysm rupture. This study sought to determine whether patients with subarachnoid hemorrhage and cerebral vasospasm were more likely to have been exposed to early hyperoxemia than those without vasospasm.
Methods: This single-center retrospective cohort study included adult patients presenting with aneurysmal subarachnoid hemorrhage to Vanderbilt University Medical Center between January 2007 and December 2017. Patients with an ICD-9/10 diagnosis of aneurysmal subarachnoid hemorrhage were initially identified (N = 441) and subsequently excluded if they did not have intracranial imaging, arterial PaO2 values or died within 96 h post-rupture (N = 96). The final cohort was 345 subjects. The degree of hyperoxemia was defined by the highest PaO2 measured within 72 h after aneurysmal rupture. The primary outcome was development of cerebral vasospasm, which included asymptomatic vasospasm and delayed cerebral ischemia (DCI). Secondary outcomes were mortality and modified Rankin Scale.
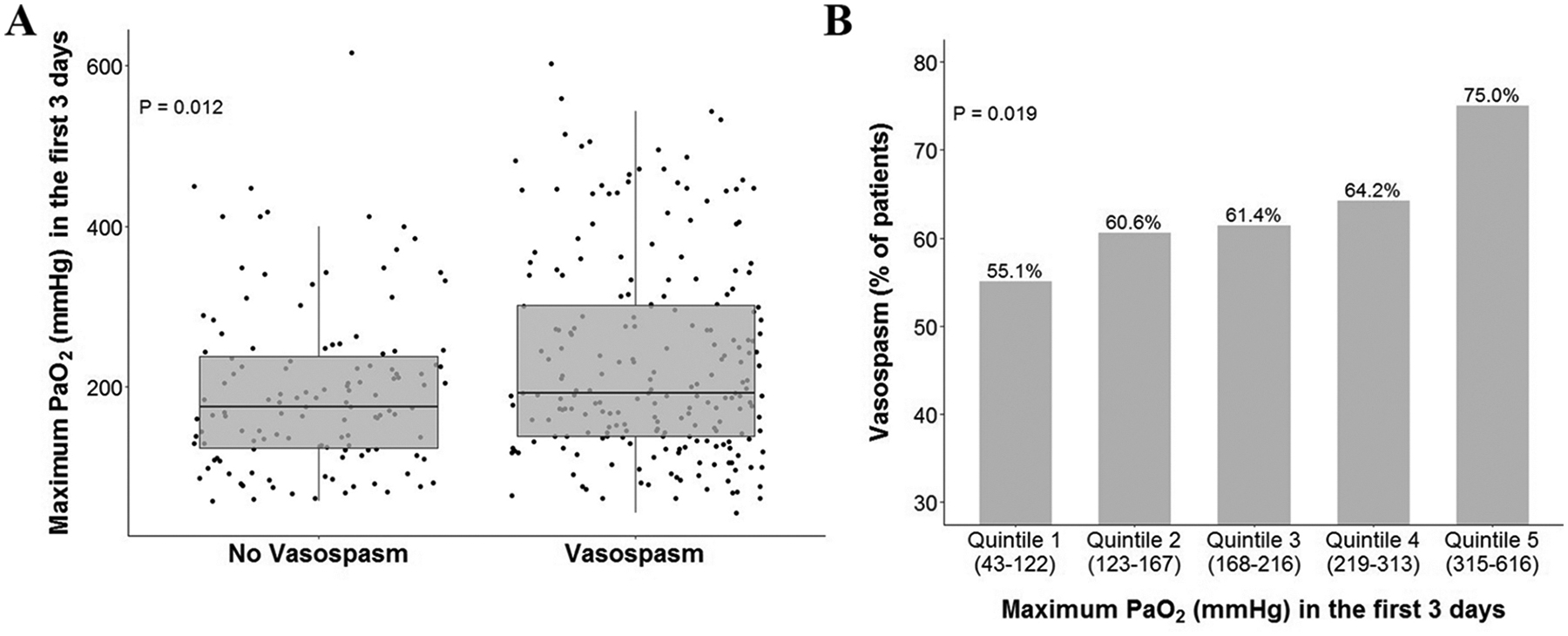
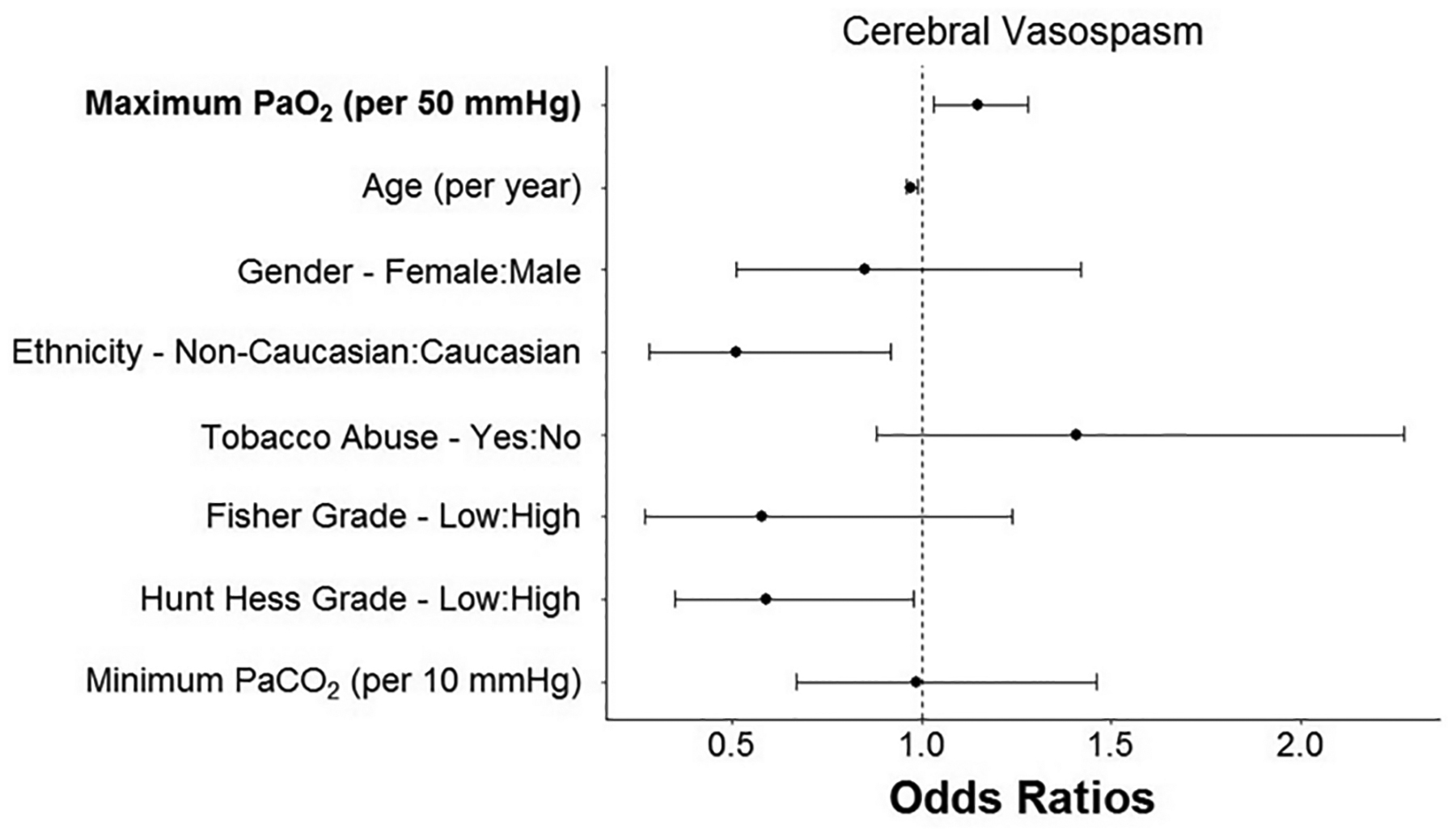
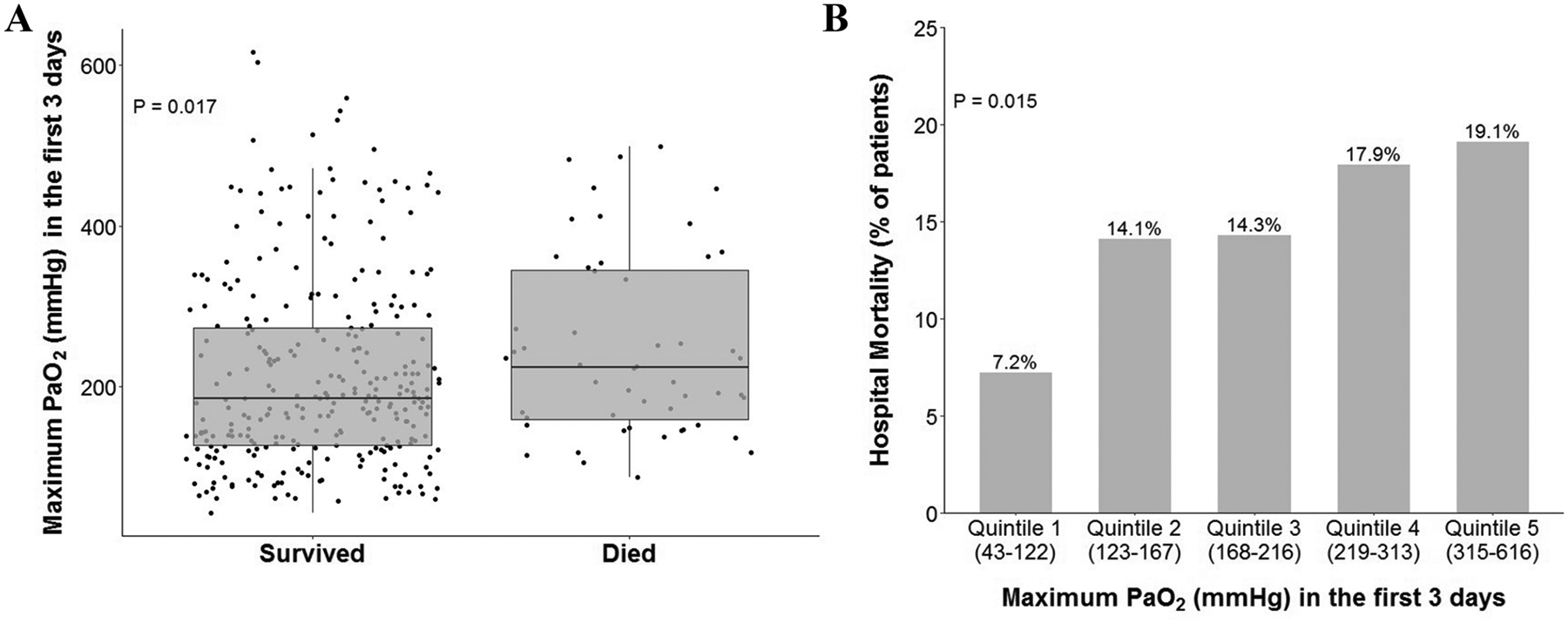
Results: Three hundred and forty five patients met inclusion criteria; 218 patients (63%) developed vasospasm. Of those that developed vasospasm, 85 were diagnosed with delayed cerebral ischemia (DCI, 39%). The average patient age of the cohort was 55 ± 13 years, and 68% were female. Ninety percent presented with Fisher grade 3 or 4 hemorrhage (N = 310), while 42% presented as Hunt-Hess grade 4 or 5 (N = 146). In univariable analysis, patients exposed to higher levels of PaO2 by quintile of exposure had a higher mortality rate and were more likely to develop vasospasm in a dose-dependent fashion (P = 0.015 and P = 0.019, respectively). There were no statistically significant predictors that differentiated asymptomatic vasospasm from DCI and no significant difference in maximum PaO2 between these two groups. In multivariable analysis, early hyperoxemia was independently associated with vasospasm (OR = 1.15 per 50 mmHg increase in PaO2 [1.03, 1.28]; P = 0.013), but not mortality (OR = 1.10 [0.97, 1.25]; P = 0.147) following subarachnoid hemorrhage.
Conclusions: Hyperoxemia within 72 h post-aneurysmal rupture is an independent predictor of cerebral vasospasm, but not mortality in subarachnoid hemorrhage. Hyperoxemia is a variable that can be readily controlled by adjusting the delivered FiO2 and may represent a modifiable risk factor for vasospasm.
Keywords: Aneurysm; Hyperoxemia; Oxidative stress; Subarachnoid hemorrhage; Vasospasm.
© 2020. Springer Science+Business Media, LLC, part of Springer Nature and Neurocritical Care Society.
Conflict of interest statement
Disclosures
Author LB Ware has received research support from Global Blood Therapeutics, CSL Behring, and Boehringer Ingelheim in the past and currently receives research support from Genentech. She also has received consulting fees from Citius, Foresee, Boehringer Ingelheim, Quark, CSL Behring and Merck. The authors have no other conflicts of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
References
-
- Vergouwen MD, Jong-Tjien-Fa AV, Algra A, et al. Time trends in causes of death after aneurysmal subarachnoid hemorrhage: A hospital-based study. Neurology. 2016;86(1):59–63. - PubMed
-
- Al-Khindi T, Macdonald RL, Schweizer TA. Cognitive and functional outcome after aneurysmal subarachnoid hemorrhage. Stroke. 2010;41(8):e519–536. - PubMed
-
- Allen GS. Role of calcium antagonists in cerebral arterial spasm. Am J Cardiol. 1985;55(3):149b–153b. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
