

Intense Simulation-Based Surgical Education for Manual Small-Incision Cataract Surgery: The Ophthalmic Learning and Improvement Initiative in Cataract Surgery Randomized Clinical Trial in Kenya, Tanzania, Uganda, and Zimbabwe
- PMID: 33151321
- PMCID: PMC7645744
- DOI: 10.1001/jamaophthalmol.2020.4718
Intense Simulation-Based Surgical Education for Manual Small-Incision Cataract Surgery: The Ophthalmic Learning and Improvement Initiative in Cataract Surgery Randomized Clinical Trial in Kenya, Tanzania, Uganda, and Zimbabwe
Abstract
Importance: Cataracts account for 40% of cases of blindness globally, with surgery the only treatment.
Objective: To determine whether adding simulation-based cataract surgical training to conventional training results in improved acquisition of surgical skills among trainees.
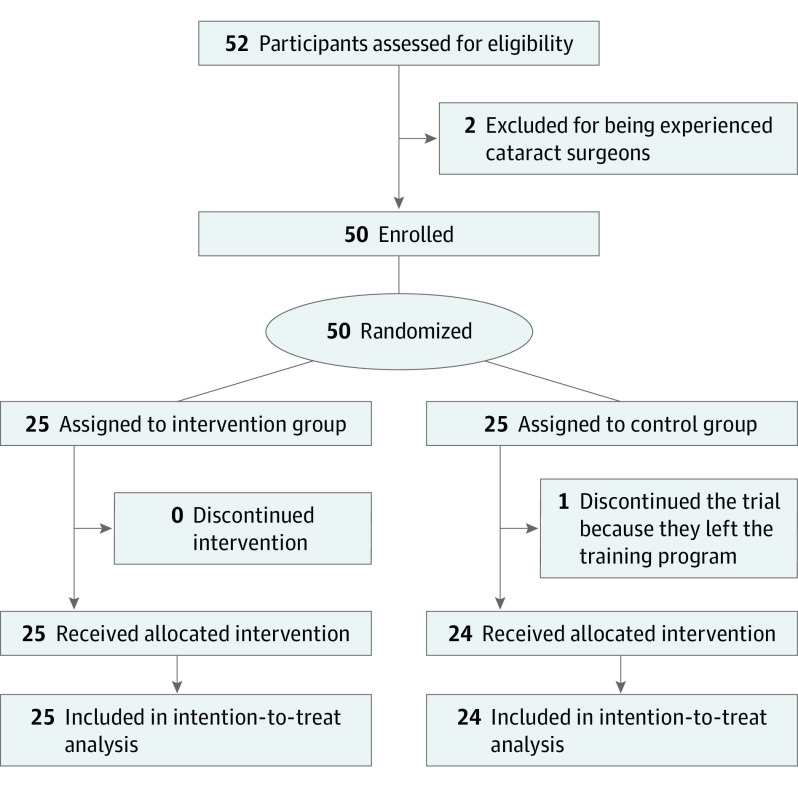
Design, setting, and participants: A multicenter, investigator-masked, parallel-group, randomized clinical educational-intervention trial was conducted at 5 university hospital training institutions in Kenya, Tanzania, Uganda, and Zimbabwe from October 1, 2017, to September 30, 2019, with a follow-up of 15 months. Fifty-two trainee ophthalmologists were assessed for eligibility (required no prior cataract surgery as primary surgeon); 50 were recruited and randomized. Those assessing outcomes of surgical competency were masked to group assignment. Analysis was performed on an intention-to-treat basis.
Interventions: The intervention group received a 5-day simulation-based cataract surgical training course, in addition to standard surgical training. The control group received standard training only, without a placebo intervention; however, those in the control group received the intervention training after the initial 12-month follow-up period.
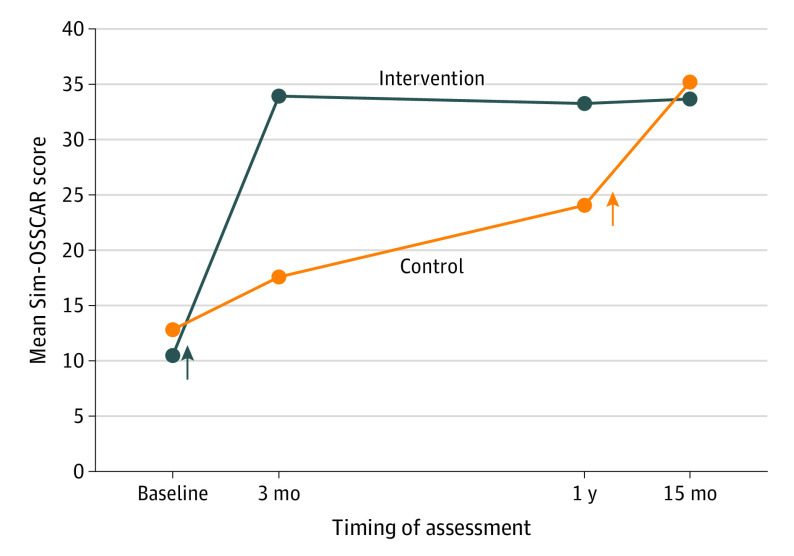
Main outcomes and measures: The primary outcome measure was overall surgical competency at 3 months, which was assessed with a validated competency assessment rubric. Secondary outcomes included surgical competence at 1 year and quantity and outcomes (including visual acuity and posterior capsule rupture) of cataract surgical procedures performed during a 1-year period.
Results: Among the 50 participants (26 women [52.0%]; mean [SD] age, 32.3 [4.6] years), 25 were randomized to the intervention group, and 25 were randomized to the control group, with 1 dropout. Forty-nine participants were included in the final intention-to-treat analysis. Baseline characteristics were balanced. The participants in the intervention group had higher scores at 3 months compared with the participants in the control group, after adjusting for baseline assessment rubric score. The participants in the intervention group were estimated to have scores 16.6 points (out of 40) higher (95% CI, 14.4-18.7; P < .001) at 3 months than the participants in the control group. The participants in the intervention group performed a mean of 21.5 cataract surgical procedures in the year after the training, while the participants in the control group performed a mean of 8.5 cataract surgical procedures (mean difference, 13.0; 95% CI, 3.9-22.2; P < .001). Posterior capsule rupture rates (an important complication) were 7.8% (42 of 537) for the intervention group and 26.6% (54 of 203) for the control group (difference, 18.8%; 95% CI, 12.3%-25.3%; P < .001).
Conclusions and relevance: This randomized clinical trial provides evidence that intense simulation-based cataract surgical education facilitates the rapid acquisition of surgical competence and maximizes patient safety.
Trial registration: Pan-African Clinical Trial Registry, number PACTR201803002159198.
Conflict of interest statement
Figures

Comment in
-
Redesigning Surgical Training Curriculum With Simulation: Lessons From the OLIMPICS Trial.JAMA Ophthalmol. 2021 Jan 1;139(1):16-17. doi: 10.1001/jamaophthalmol.2020.4716. JAMA Ophthalmol. 2021. PMID: 33151270 No abstract available.
References
-
- Flaxman SR, Bourne RRA, Resnikoff S, et al. ; Vision Loss Expert Group of the Global Burden of Disease Study . Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221-e1234. doi:10.1016/S2214-109X(17)30393-5 - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
