

Glioblastoma post-operative imaging in neuro-oncology: current UK practice (GIN CUP study)
- PMID: 33151394
- PMCID: PMC8043861
- DOI: 10.1007/s00330-020-07387-3
Glioblastoma post-operative imaging in neuro-oncology: current UK practice (GIN CUP study)
Abstract
Objectives: MRI remains the preferred imaging investigation for glioblastoma. Appropriate and timely neuroimaging in the follow-up period is considered to be important in making management decisions. There is a paucity of evidence-based information in current UK, European and international guidelines regarding the optimal timing and type of neuroimaging following initial neurosurgical treatment. This study assessed the current imaging practices amongst UK neuro-oncology centres, thus providing baseline data and informing future practice.
Methods: The lead neuro-oncologist, neuroradiologist and neurosurgeon from every UK neuro-oncology centre were invited to complete an online survey. Participants were asked about current and ideal imaging practices following initial treatment.
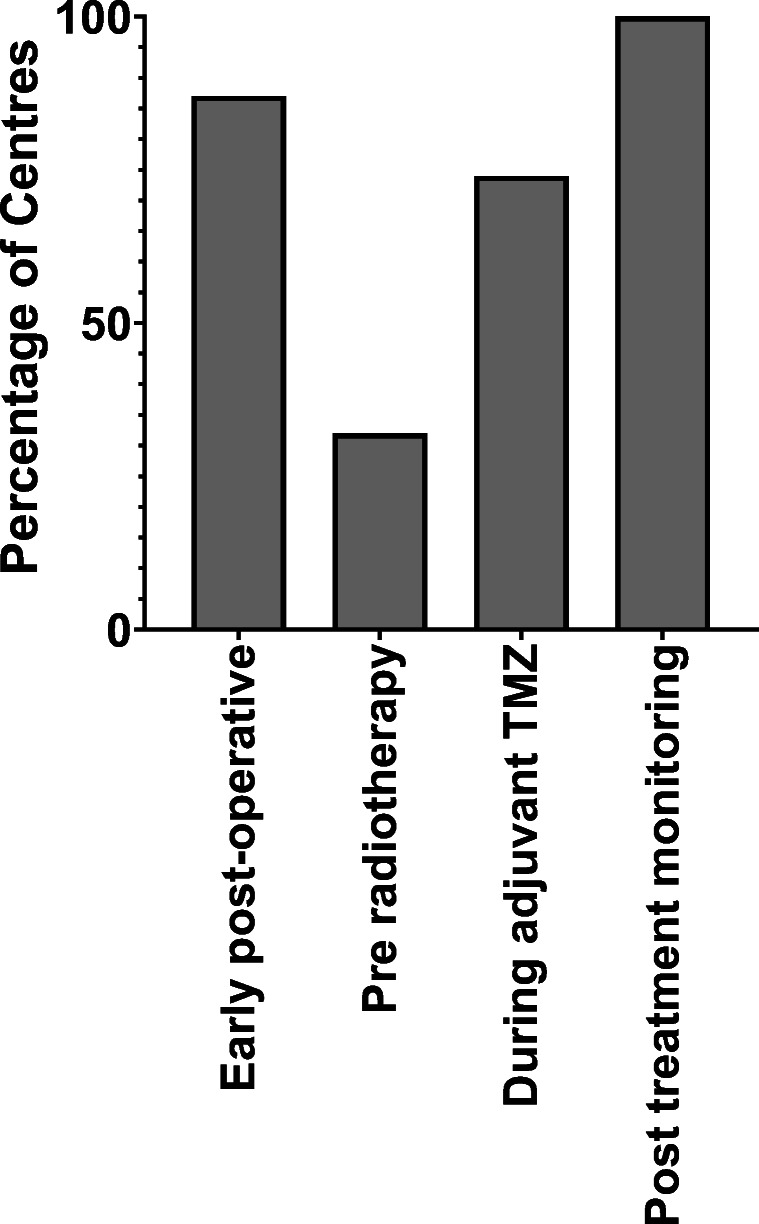
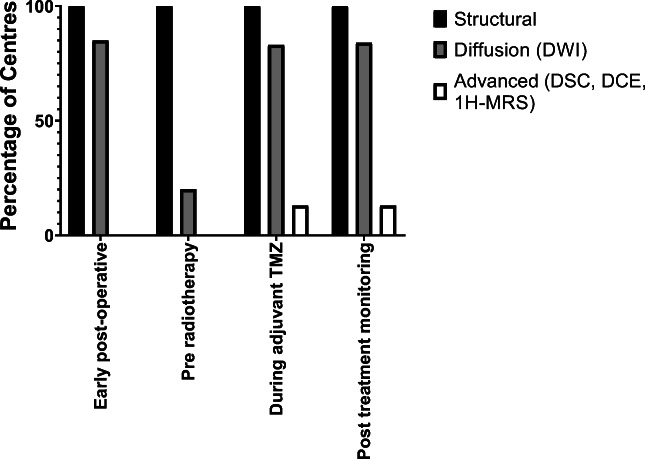
Results: Ninety-two participants from all 31 neuro-oncology centres completed the survey (100% response rate). Most centres routinely performed an early post-operative MRI (87%, 27/31), whereas only a third performed a pre-radiotherapy MRI (32%, 10/31). The number and timing of scans routinely performed during adjuvant TMZ treatment varied widely between centres. At the end of the adjuvant period, most centres performed an MRI (71%, 22/31), followed by monitoring scans at 3 monthly intervals (81%, 25/31). Additional short-interval imaging was carried out in cases of possible pseudoprogression in most centres (71%, 22/31). Routine use of advanced imaging was infrequent; however, the addition of advanced sequences was the most popular suggestion for ideal imaging practice, followed by changes in the timing of EPMRI.
Conclusion: Variations in neuroimaging practices exist after initial glioblastoma treatment within the UK. Multicentre, longitudinal, prospective trials are needed to define the optimal imaging schedule for assessment.
Key points: • Variations in imaging practices exist in the frequency, timing and type of interval neuroimaging after initial treatment of glioblastoma within the UK. • Large, multicentre, longitudinal, prospective trials are needed to define the optimal imaging schedule for assessment.
Keywords: Glioblastoma; Guideline; Neuroimaging; Survey.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
-
- Brodbelt A, Greenberg D, Winters T et al (2015) Glioblastoma in England: 2007-2011. Eur J Cancer 51(4):533–542 - PubMed
-
- Stupp R, Mason WP, van den Bent MJ et al (2005) Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352(10):987–996 - PubMed
-
- Stupp R, Hegi ME, Mason WP et al (2009) Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 10(5):459–466 - PubMed
-
- Sanghera P, Rampling R, Haylock B et al (2012) The concepts, diagnosis and management of early imaging changes after therapy for glioblastomas. Clin Oncol (R Coll Radiol) 24(3):216–227 - PubMed
-
- British Society of Neuroradiologists (2018) Core imaging protocol for brain tumours. British Society of Neuroradiologists, UK. Available from: https://bsnr.org.uk/_userfiles/pages/files/bsnrstandardsbraintumour.pdf. Accessed Jan 2019
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
