

Baroreflex responses during dry resting and exercise apnoeas in air and pure oxygen
- PMID: 33151437
- PMCID: PMC7862076
- DOI: 10.1007/s00421-020-04544-w
Baroreflex responses during dry resting and exercise apnoeas in air and pure oxygen
Abstract
Purpose: We analysed the characteristics of arterial baroreflexes during the first phase of apnoea (φ1).
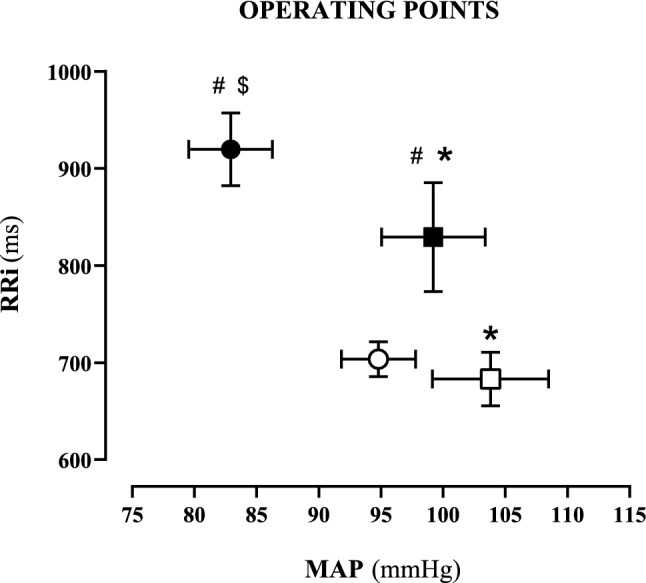
Methods: 12 divers performed rest and exercise (30 W) apnoeas (air and oxygen). We measured beat-by-beat R-to-R interval (RRi) and mean arterial pressure (MAP). Mean RRi and MAP values defined the operating point (OP) before (PRE-ss) and in the second phase (φ2) of apnoea. Baroreflex sensitivity (BRS, ms·mmHg-1) was calculated with the sequence method.
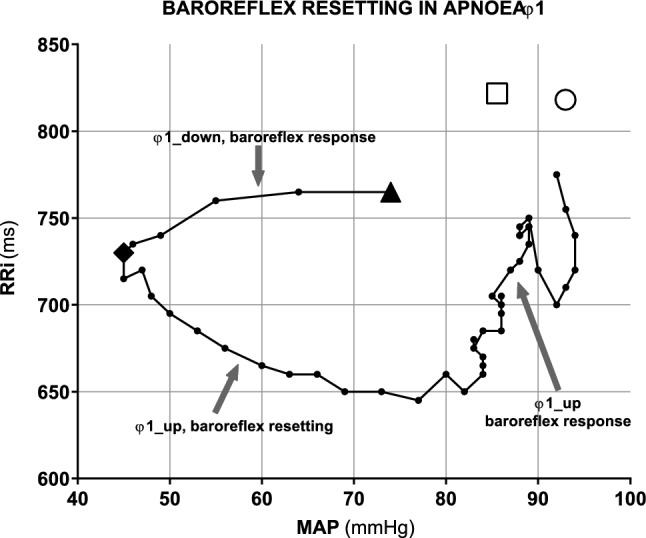
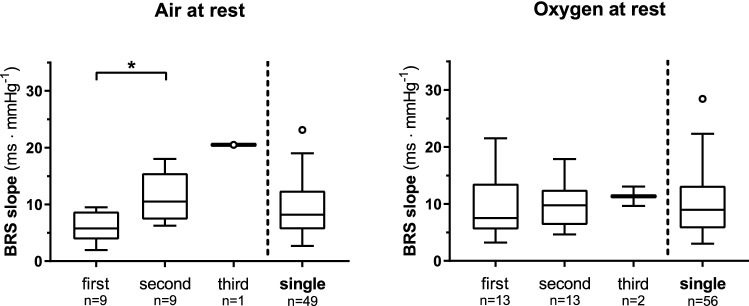
Results: In PRE-ss, BRS was (median [IQR]): at rest, 20.3 [10.0-28.6] in air and 18.8 [13.8-25.2] in O2; at exercise 9.2[8.4-13.2] in air and 10.1[8.4-13.6] in O2. In φ1, during MAP decrease, BRS was lower than in PRE-ss at rest (6.6 [5.3-11.4] in air and 7.7 [4.9-14.3] in O2, p < 0.05). At exercise, BRS in φ1 was 6.4 [3.9-13.1] in air and 6.7 [4.1-9.5] in O2. After attainment of minimum MAP (MAPmin), baroreflex resetting started. After attainment of minimum RRi, baroreflex sequences reappeared. In φ2, BRS at rest was 12.1 [9.6-16.2] in air, 12.9 [9.2-15.8] in O2. At exercise (no φ2 in air), it was 7.9 [5.4-10.7] in O2. In φ2, OP acts at higher MAP values.
Conclusion: In apnoea φ1, there is a sudden correction of MAP fall via baroreflex. The lower BRS in the earliest φ1 suggests a possible parasympathetic mechanism underpinning this reduction. After MAPmin, baroreflex resets, displacing its OP at higher MAP level; thus, resetting may not be due to central command. After resetting, restoration of BRS suggests re-establishment of vagal drive.
Keywords: Baroreflex resetting; Baroreflex sensitivity; Breath holding; Closed loop; Sequence method.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Dynamics of cardiovascular and baroreflex readjustments during a light-to-moderate exercise transient in humans.Eur J Appl Physiol. 2022 Nov;122(11):2343-2354. doi: 10.1007/s00421-022-05011-4. Epub 2022 Jul 21. Eur J Appl Physiol. 2022. PMID: 35861802 Free PMC article.
-
Baroreflex dynamics during the rest to exercise transient in acute normobaric hypoxia in humans.Eur J Appl Physiol. 2024 Sep;124(9):2765-2775. doi: 10.1007/s00421-024-05485-4. Epub 2024 Apr 24. Eur J Appl Physiol. 2024. PMID: 38656378 Free PMC article.
-
A closed-loop approach to the study of the baroreflex dynamics during posture changes at rest and at exercise in humans.Am J Physiol Regul Integr Comp Physiol. 2021 Dec 1;321(6):R960-R968. doi: 10.1152/ajpregu.00167.2021. Epub 2021 Oct 13. Am J Physiol Regul Integr Comp Physiol. 2021. PMID: 34643104
-
Human investigations into the arterial and cardiopulmonary baroreflexes during exercise.Exp Physiol. 2012 Jan;97(1):39-50. doi: 10.1113/expphysiol.2011.057554. Epub 2011 Oct 14. Exp Physiol. 2012. PMID: 22002871 Free PMC article. Review.
-
Central baroreflex resetting as a means of increasing and decreasing sympathetic outflow and arterial pressure.Ann N Y Acad Sci. 2001 Jun;940:324-37. doi: 10.1111/j.1749-6632.2001.tb03688.x. Ann N Y Acad Sci. 2001. PMID: 11458690 Review.
Cited by
-
A century of exercise physiology: key concepts on coupling respiratory oxygen flow to muscle energy demand during exercise.Eur J Appl Physiol. 2022 Jun;122(6):1317-1365. doi: 10.1007/s00421-022-04901-x. Epub 2022 Feb 26. Eur J Appl Physiol. 2022. PMID: 35217911 Free PMC article. Review.
-
A systematic review of HRV during diving in very cold water.Int J Circumpolar Health. 2023 Dec;82(1):2203369. doi: 10.1080/22423982.2023.2203369. Int J Circumpolar Health. 2023. PMID: 37079282 Free PMC article.
-
Energetics of Underwater Swimming in Apnea.Med Sci Sports Exerc. 2025 Sep 1;57(9):2053-2061. doi: 10.1249/MSS.0000000000003731. Epub 2025 Apr 15. Med Sci Sports Exerc. 2025. PMID: 40231725 Free PMC article.
-
Dynamics of cardiovascular and baroreflex readjustments during a light-to-moderate exercise transient in humans.Eur J Appl Physiol. 2022 Nov;122(11):2343-2354. doi: 10.1007/s00421-022-05011-4. Epub 2022 Jul 21. Eur J Appl Physiol. 2022. PMID: 35861802 Free PMC article.
-
Baroreflex dynamics during the rest to exercise transient in acute normobaric hypoxia in humans.Eur J Appl Physiol. 2024 Sep;124(9):2765-2775. doi: 10.1007/s00421-024-05485-4. Epub 2024 Apr 24. Eur J Appl Physiol. 2024. PMID: 38656378 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
