

Imaging of calcific tendinopathy around the shoulder: usual and unusual presentations and common pitfalls
- PMID: 33151457
- PMCID: PMC8007494
- DOI: 10.1007/s11547-020-01300-0
Imaging of calcific tendinopathy around the shoulder: usual and unusual presentations and common pitfalls
Abstract
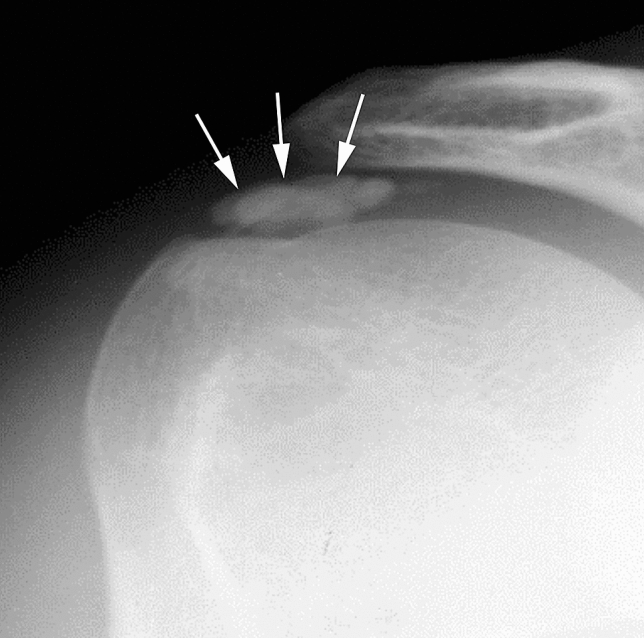
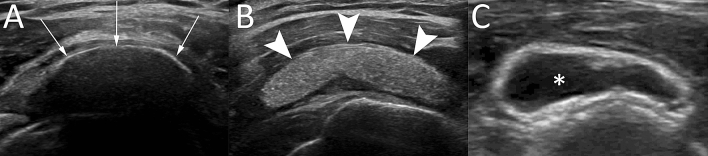
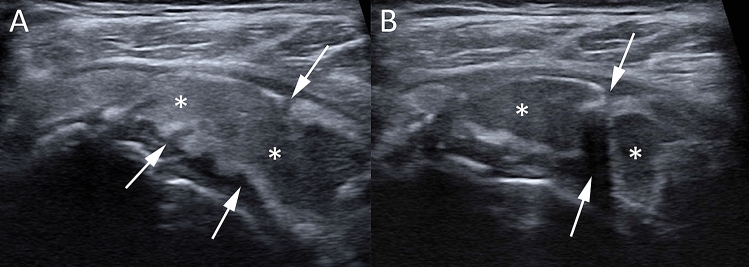
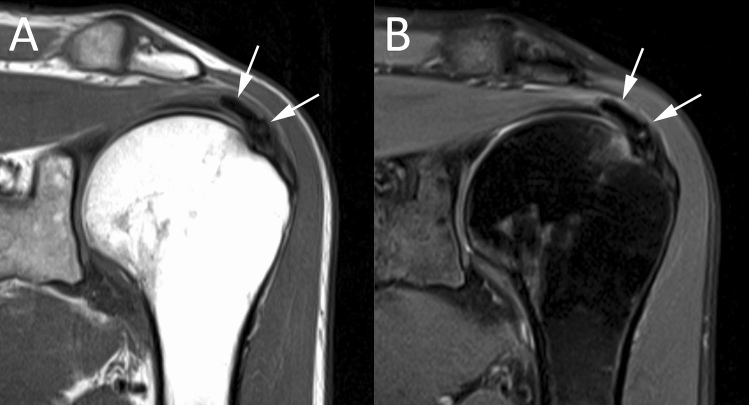
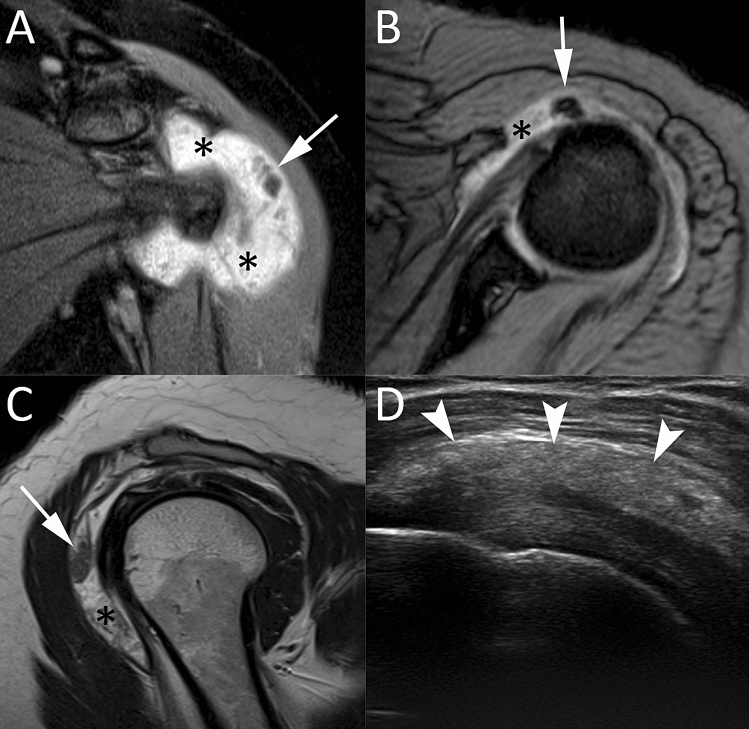
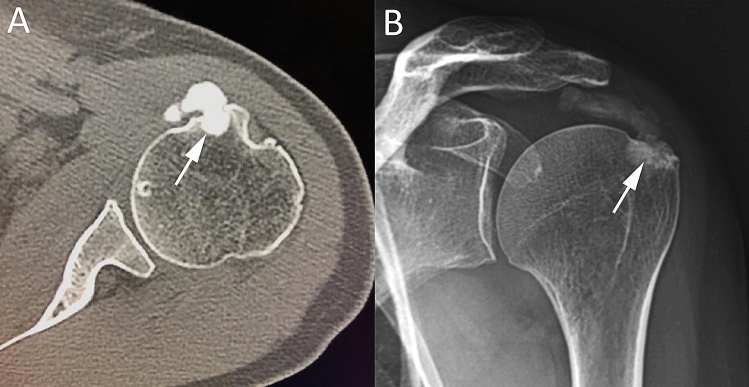
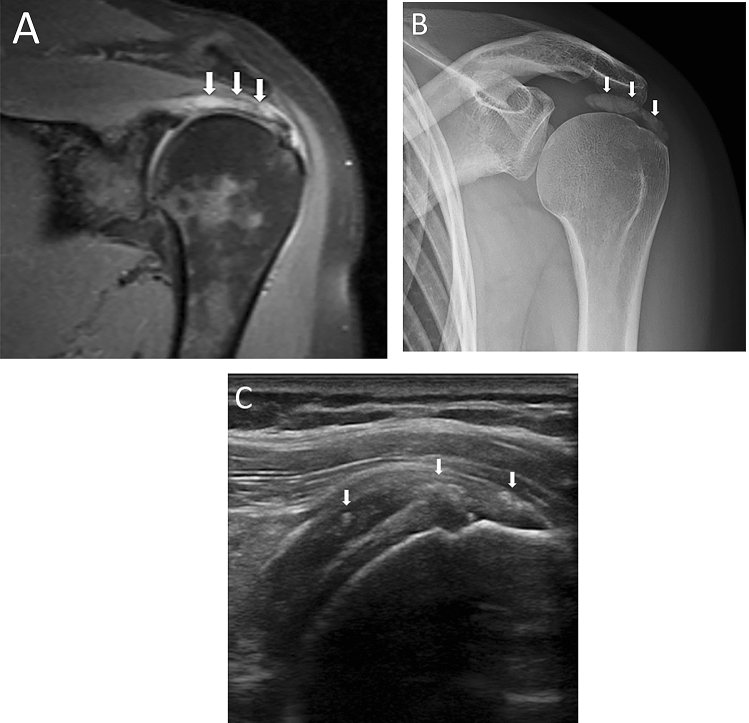
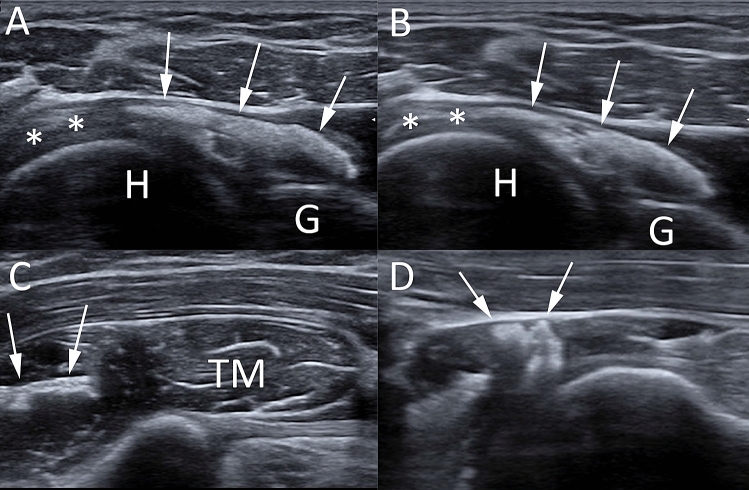
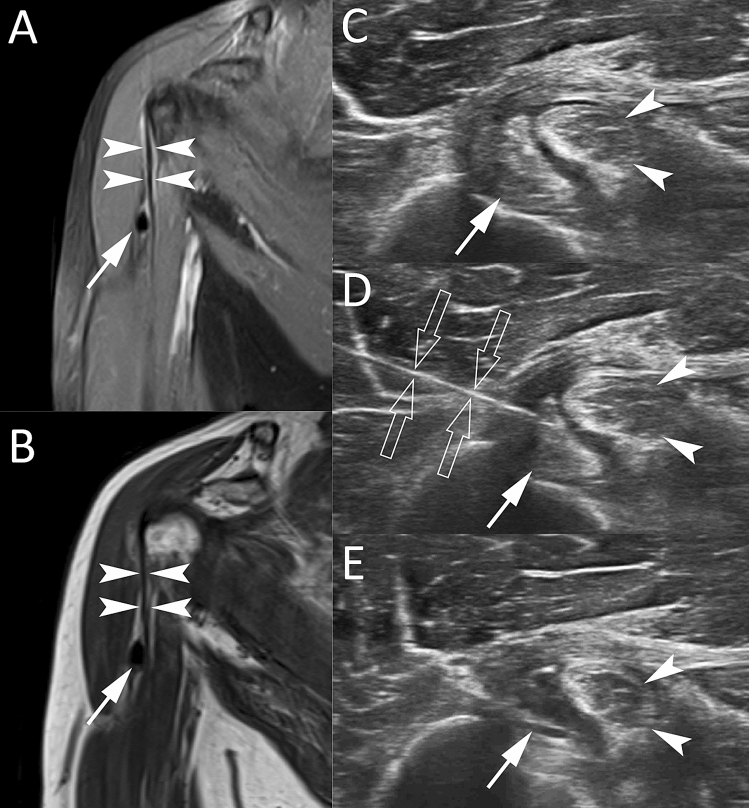
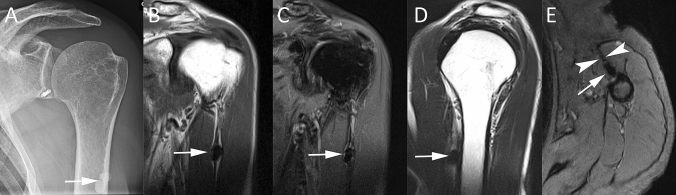
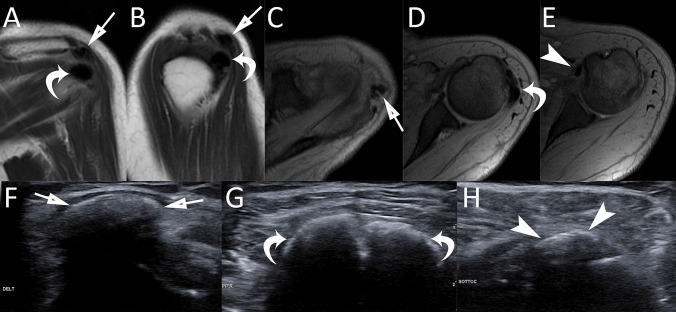
Rotator cuff calcific tendinopathy (RCCT) is a very common condition, characterized by calcium deposition over fibrocartilaginous metaplasia of tenocytes, mainly occurring in the supraspinatus tendon. RCCT has a typical imaging presentation: in most cases, calcific deposits appear as a dense opacity around the humeral head on conventional radiography, as hyperechoic foci with or without acoustic shadow at ultrasound and as a signal void at magnetic resonance imaging. However, radiologists have to keep in mind the possible unusual presentations of RCCT and the key imaging features to correctly differentiate RCCT from other RC conditions, such as calcific enthesopathy or RC tears. Other presentations of RCCT to be considered are intrabursal, intraosseous, and intramuscular migration of calcific deposits that may mimic infectious processes or malignancies. While intrabursal and intraosseous migration are quite common, intramuscular migration is an unusual evolution of RCCT. It is important also to know atypical regions affected by calcific tendinopathy as biceps brachii, pectoralis major, and deltoid tendons. Unusual presentations of RCCT may lead to diagnostic challenge and mistakes. The aim of this review is to illustrate the usual and unusual imaging findings of RCCT that radiologists should know to reach the correct diagnosis and to exclude other entities with the purpose of preventing further unnecessary imaging examinations or interventional procedures.
Keywords: Calcific tendinopathy; Conventional radiography; Magnetic resonance; Pitfall; Rotator cuff; Ultrasound.
Conflict of interest statement
Authors declare that they have no conflict of interest.
Figures

Similar articles
-
Zero echo time MRI in shoulder MRI protocols for the diagnosis of rotator cuff calcific tendinopathy improves identification of calcific deposits compared to conventional MR sequences but remains sub-optimal compared to radiographs.Eur Radiol. 2023 Sep;33(9):6381-6391. doi: 10.1007/s00330-023-09602-3. Epub 2023 Apr 4. Eur Radiol. 2023. PMID: 37014406
-
Rotator cuff calcific tendinopathy: from diagnosis to treatment.Acta Biomed. 2018 Jan 19;89(1-S):186-196. doi: 10.23750/abm.v89i1-S.7022. Acta Biomed. 2018. PMID: 29350647 Free PMC article. Review.
-
Intramuscular migration of calcium deposits into the deltoid muscle: two cases of a rare complication of rotator cuff calcific tendinopathy.J Ultrasound. 2023 Dec;26(4):929-933. doi: 10.1007/s40477-023-00786-4. Epub 2023 May 24. J Ultrasound. 2023. PMID: 37222926 Free PMC article.
-
Calcific tendinopathy of the shoulder with intraosseous extension: outcomes of ultrasound-guided percutaneous irrigation.Skeletal Radiol. 2017 Feb;46(2):201-208. doi: 10.1007/s00256-016-2538-9. Epub 2016 Dec 1. Skeletal Radiol. 2017. PMID: 27909786
-
Intramuscular migration of calcific tendinopathy in the rotator cuff: ultrasound appearance and a review of the literature.J Ultrasound. 2016 Mar 25;19(3):175-81. doi: 10.1007/s40477-016-0202-9. eCollection 2016 Sep. J Ultrasound. 2016. PMID: 27635162 Free PMC article. Review.
Cited by
-
Can Secondary Adhesive Capsulitis Complicate Calcific Tendinitis of the Rotator Cuff? An Ultrasound Imaging Analysis.Clin Pract. 2024 Mar 28;14(2):579-589. doi: 10.3390/clinpract14020045. Clin Pract. 2024. PMID: 38666803 Free PMC article.
-
Ultrasound-guided percutaneous irrigation of rotator cuff calcific tendinosis. What radiologist should know.Pol J Radiol. 2022 Feb 13;87:e87-e92. doi: 10.5114/pjr.2022.113491. eCollection 2022. Pol J Radiol. 2022. PMID: 35280948 Free PMC article. Review.
-
Ultrasound-guided percutaneous irrigation of calcific tendinopathy outside the rotator cuff: short-term evaluation.Skeletal Radiol. 2022 Oct;51(10):2039-2044. doi: 10.1007/s00256-022-04035-3. Epub 2022 Apr 2. Skeletal Radiol. 2022. PMID: 35366095
-
Chronic intramuscular calcific tendinitis of the deltoid muscle.Skeletal Radiol. 2023 Jun;52(6):1251-1256. doi: 10.1007/s00256-022-04203-5. Epub 2022 Oct 12. Skeletal Radiol. 2023. PMID: 36224399
-
Zero echo time MRI in shoulder MRI protocols for the diagnosis of rotator cuff calcific tendinopathy improves identification of calcific deposits compared to conventional MR sequences but remains sub-optimal compared to radiographs.Eur Radiol. 2023 Sep;33(9):6381-6391. doi: 10.1007/s00330-023-09602-3. Epub 2023 Apr 4. Eur Radiol. 2023. PMID: 37014406
References
-
- Bosworth B. Calcium deposits in the shoulder and subacromial bursitis: a survey of 12,122 shoulders. J Am Med Assoc. 1941;116:2477–2482. doi: 10.1001/jama.1941.02820220019004. - DOI
