

Cardiometabolic risk factors and survival after cancer in the Women's Health Initiative
- PMID: 33151547
- PMCID: PMC10448774
- DOI: 10.1002/cncr.33295
Cardiometabolic risk factors and survival after cancer in the Women's Health Initiative
Abstract
Background: Cardiometabolic abnormalities are a leading cause of death among women, including women with cancer.
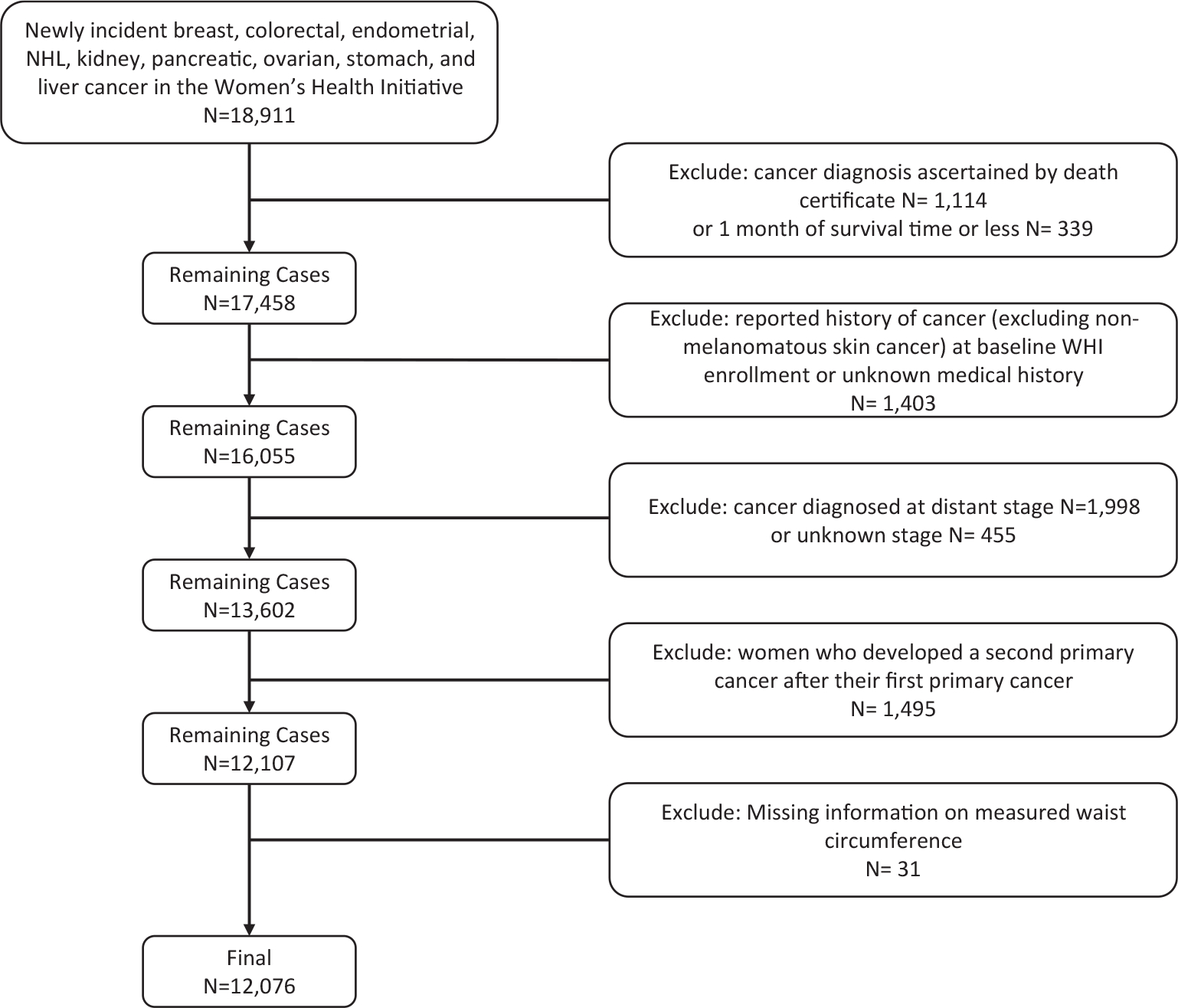
Methods: This study examined the association between prediagnosis cardiovascular health and total and cause-specific mortality among 12,076 postmenopausal women who developed local- or regional-stage invasive cancer in the Women's Health Initiative (WHI). Cardiovascular risk factors included waist circumference, hypertension, high cholesterol, and type 2 diabetes. Obesity-related cancers included breast cancer, colorectal cancer, endometrial cancer, kidney cancer, pancreatic cancer, ovarian cancer, stomach cancer, liver cancer, and non-Hodgkin lymphoma. Cox proportional hazards models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) adjusted for important predictors of survival.
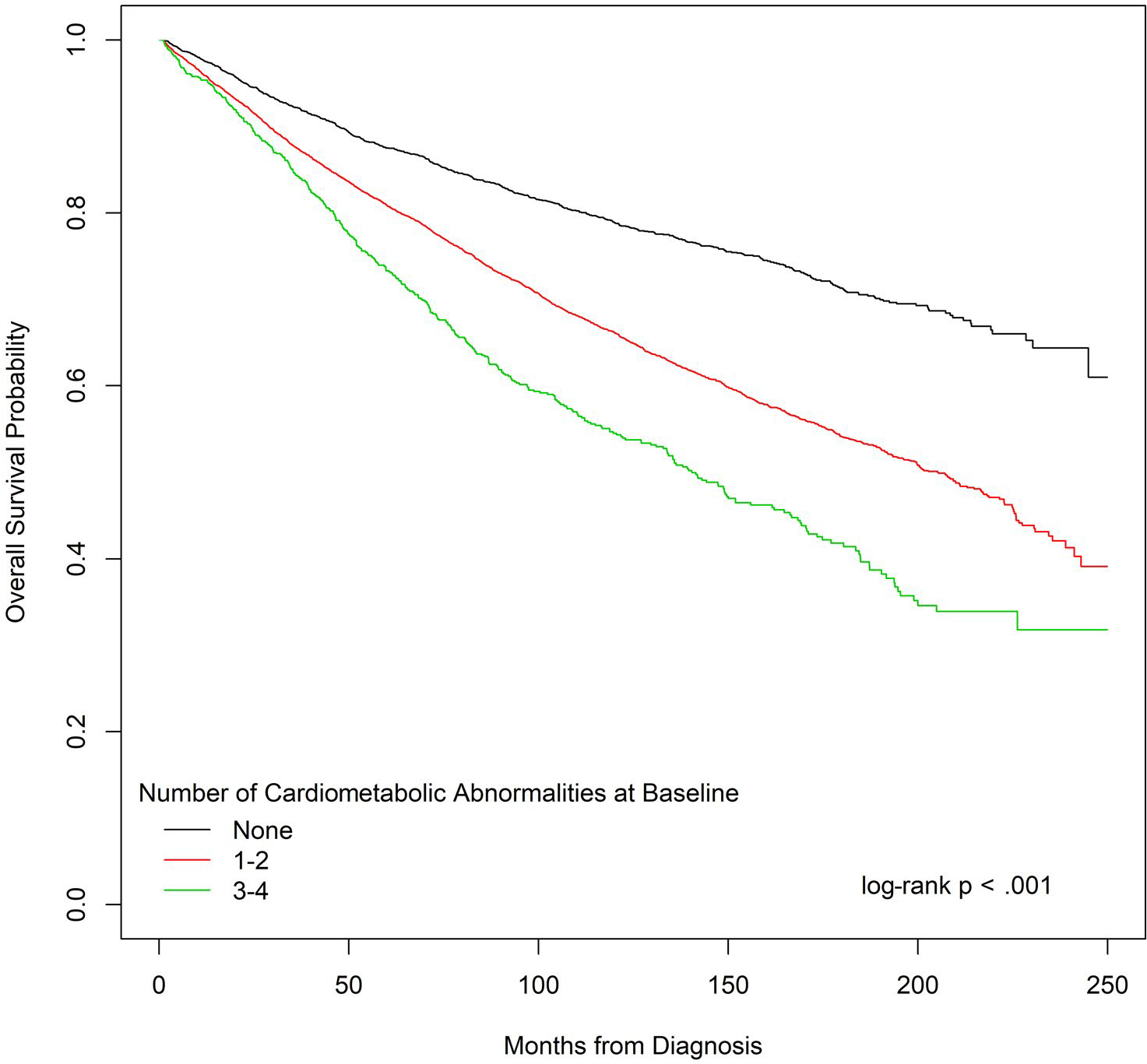
Results: After a median follow-up of 10.0 years from the date of the cancer diagnosis, there were 3607 total deaths, with 1546 (43%) due to cancer. Most participants (62.9%) had 1 or 2 cardiometabolic risk factors, and 8.1% had 3 or 4. In adjusted models, women with 3 to 4 risk factors (vs none) had a higher risk of all-cause mortality (HR, 1.99; 95% CI, 1.73-2.30), death due to cardiovascular disease (CVD) (HR, 4.01; 95% CI, 2.88-5.57), cancer-specific mortality (HR, 1.37; 95% CI, 1.1-1.72), and other-cause mortality (HR, 2.14; 95% CI, 1.70-2.69). A higher waist circumference was associated with greater all-cause mortality (HR, 1.17; 95% CI, 1.06-1.30) and cancer-specific mortality (HR, 1.22; 95% CI, 1.04-1.42).
Conclusions: Among postmenopausal women diagnosed with cancer in the WHI, cardiometabolic risk factors before the cancer diagnosis were associated with greater all-cause, CVD, cancer-specific, and other-cause mortality. These results raise hypotheses regarding potential clinical intervention strategies targeting cardiometabolic abnormalities that require future prospective studies for confirmation.
Lay summary: This study uses information from the Women's Health Initiative (WHI) to find out whether cardiac risk factors are related to a greater risk of dying among older women with cancer. The WHI is the largest study of medical problems faced by older women in this country. The results show that women who have 3 or 4 risk factors are more likely to die of any cause, heart disease, or cancer in comparison with women with no risk factors. It is concluded that interventions to help to lower the burden of cardiac risk factors can have an important impact on survivorship among women with cancer.
Keywords: Women's Health Initiative; cancer; cardiometabolic risk factors; survival.
© 2020 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
Michael S. Simon reports personal fees from the Women’s Health Initiative during the conduct of the study and that he is on a speakers’ bureau for AstraZeneca for non–treatment-related genetic counseling and testing. Theresa A. Hastert reports personal fees from the Women’s Health Initiative during the conduct of the study and grants from the American Cancer Society and the National Cancer Institute outside the submitted work. Ana Barac reports working on a data and safety monitoring board for CTI Biopharma and receiving honoraria from Bristol-Myers Squibb. Rowan T. Chlebowski reports personal fees from Novartis, Pfizer, AstraZeneca, Puma, Genentech, Immunomedics, and Merck during the conduct of the study. Aladdin H. Shadyab reports working as a consultant for Ranchio Biosciences, LLC. The other authors made no disclosures.
Figures
References
-
- Ahmadi A, Leipsic J, Feuchtner G, et al. Is metabolic syndrome predictive of prevalence, extent, and risk of coronary artery disease beyond its components? Results from the multinational coronary CT angiography evaluation for clinical outcome: an international multicenter registry (CONFIRM). PLoS One. 2015;10:e0118998. - PMC - PubMed
-
- O’Neill S, O’Driscoll L. Metabolic syndrome: a closer look at the growing epidemic and its associated pathologies. Obes Rev. 2015;16:1–12. - PubMed
-
- Lakka HM, Laaksonen DE, Lakka TA, et al. The metabolic syndrome and total and cardiovascular disease mortality in middle-aged men. JAMA. 2002;288:2709–2716. - PubMed
-
- Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120:1640–1645. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 DK062290/DK/NIDDK NIH HHS/United States
- UM1 CA173642/CA/NCI NIH HHS/United States
- 32100-2/HL/NHLBI NIH HHS/United States
- 42129-32/HL/NHLBI NIH HHS/United States
- N01 WH022110/WH/WHI NIH HHS/United States
- 32111-13/HL/NHLBI NIH HHS/United States
- N01WH22110/HL/NHLBI NIH HHS/United States
- U01 CA173642/CA/NCI NIH HHS/United States
- 24152/HL/NHLBI NIH HHS/United States
- 32122/HL/NHLBI NIH HHS/United States
- 44221/HL/NHLBI NIH HHS/United States
- R21 CA100720/CA/NCI NIH HHS/United States
- 32108-9/HL/NHLBI NIH HHS/United States
- R21 DK084452/DK/NIDDK NIH HHS/United States
- 32118-32119/HL/NHLBI NIH HHS/United States
- 32105-6/HL/NHLBI NIH HHS/United States
- P30 CA022453/CA/NCI NIH HHS/United States
- 32115/HL/NHLBI NIH HHS/United States
- 42107-26/HL/NHLBI NIH HHS/United States
