

Evaluation of an intervention to provide brief support and personalized feedback on food shopping to reduce saturated fat intake (PC-SHOP): A randomized controlled trial
- PMID: 33151934
- PMCID: PMC7643942
- DOI: 10.1371/journal.pmed.1003385
Evaluation of an intervention to provide brief support and personalized feedback on food shopping to reduce saturated fat intake (PC-SHOP): A randomized controlled trial
Abstract
Background: Guidelines recommend reducing saturated fat (SFA) intake to decrease cardiovascular disease (CVD) risk, but there is limited evidence on scalable and effective approaches to change dietary intake, given the large proportion of the population exceeding SFA recommendations. We aimed to develop a system to provide monthly personalized feedback and healthier swaps based on nutritional analysis of loyalty card data from the largest United Kingdom grocery store together with brief advice and support from a healthcare professional (HCP) in the primary care practice. Following a hybrid effectiveness-feasibility design, we tested the effects of the intervention on SFA intake and low-density lipoprotein (LDL) cholesterol as well as the feasibility and acceptability of providing nutritional advice using loyalty card data.
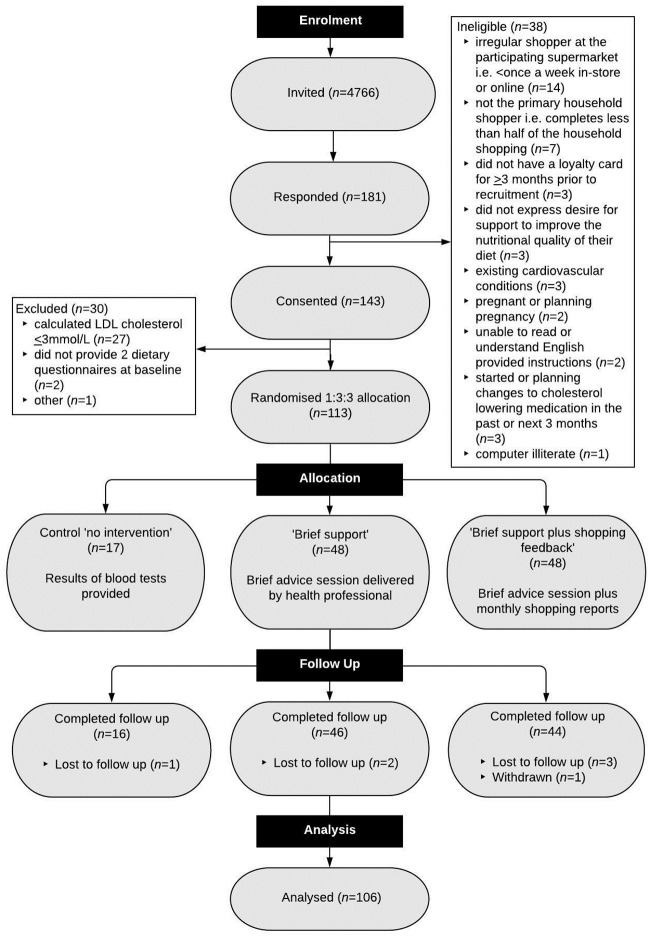
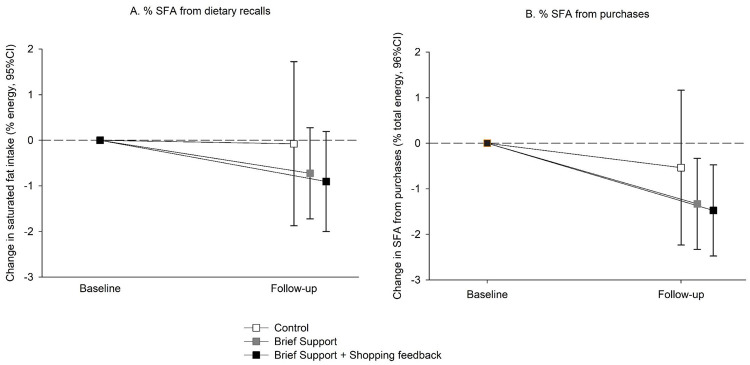
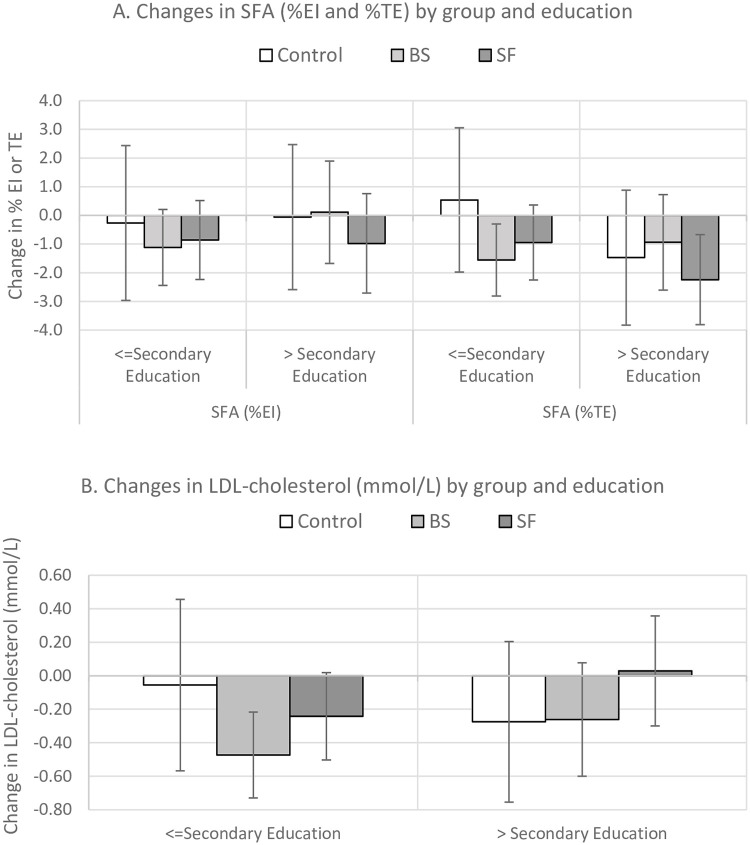
Methods and findings: The Primary Care Shopping Intervention for Cardiovascular Disease Prevention (PC-SHOP) study is a parallel randomized controlled trial with a 3 month follow-up conducted between 21 March 2018 to 16 January2019. Adults ≥18 years with LDL cholesterol >3 mmol/L (n = 113) were recruited from general practitioner (GP) practices in Oxfordshire and randomly allocated to "Brief Support" (BS, n = 48), "Brief Support + Shopping Feedback" (SF, n = 48) or "Control" (n = 17). BS consisted of a 10-minute consultation with an HCP to motivate participants to reduce their SFA intake. Shopping feedback comprised a personalized report on the SFA content of grocery purchases and suggestions for lower SFA swaps. The primary outcome was the between-group difference in change in SFA intake (% total energy intake) at 3 months adjusted for baseline SFA and GP practice using intention-to-treat analysis. Secondary outcomes included %SFA in purchases, LDL cholesterol, and feasibility outcomes. The trial was powered to detect an absolute reduction in SFA of 3% (SD3). Neither participants nor the study team were blinded to group allocation. A total of 106 (94%) participants completed the study: 68% women, 95% white ethnicity, average age 62.4 years (SD 10.8), body mass index (BMI) 27.1 kg/m2 (SD 4.7). There were small decreases in SFA intake at 3 months: control = -0.1% (95% CI -1.8 to 1.7), BS = -0.7% (95% CI -1.8 to 0.3), SF = -0.9% (95% CI -2.0 to 0.2); but no evidence of a significant effect of either intervention compared with control (difference adjusted for GP practice and baseline: BS versus control = -0.33% [95% CI -2.11 to 1.44], p = 0.709; SF versus control = -0.11% [95% CI -1.92 to 1.69], p = 0.901). There were similar trends in %SFA based on supermarket purchases: control = -0.5% (95% CI -2.3 to 1.2), BS = -1.3% (95% CI -2.3 to -0.3), SF = -1.5% (95% CI -2.5 to -0.5) from baseline to follow-up, but these were not significantly different: BS versus control p = 0.379; SF versus control p = 0.411. There were small reductions in LDL from baseline to follow-up (control = -0.14 mmol/L [95% CI -0.48, 0.19), BS: -0.39 mmol/L [95% CI -0.59, -0.19], SF: -0.14 mmol/L [95% CI -0.34, 0.07]), but these were not significantly different: BS versus control p = 0.338; SF versus control p = 0.790. Limitations of this study include the small sample of participants recruited, which limits the power to detect smaller differences, and the low response rate (3%), which may limit the generalisability of these findings.
Conclusions: In this study, we have shown it is feasible to deliver brief advice in primary care to encourage reductions in SFA intake and to provide personalized advice to encourage healthier choices using supermarket loyalty card data. There was no evidence of large reductions in SFA, but we are unable to exclude more modest benefits. The feasibility, acceptability, and scalability of these interventions suggest they have potential to encourage small changes in diet, which could be beneficial at the population level.
Trial registration: ISRCTN14279335.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- England PH. National Diet and Nutrition Survey: Results from years 7 and 8 (combined) 2018.
-
- Pot GK, Prynne CJ, Roberts C, Olson A, Nicholson SK, Whitton C, et al. National Diet and Nutrition Survey: fat and fatty acid intake from the first year of the rolling programme and comparison with previous surveys. British journal of nutrition. 2012;107(3):405–15. 10.1017/S0007114511002911 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
