

A multivariable prognostic score to guide systemic therapy in early-stage HER2-positive breast cancer: a retrospective study with an external evaluation
- PMID: 33152285
- PMCID: PMC8140650
- DOI: 10.1016/S1470-2045(20)30450-2
A multivariable prognostic score to guide systemic therapy in early-stage HER2-positive breast cancer: a retrospective study with an external evaluation
Abstract
Background: In early-stage HER2-positive breast cancer, escalation or de-escalation of systemic therapy is a controversial topic. As an aid to treatment decisions, we aimed to develop a prognostic assay that integrates multiple data types for predicting survival outcome in patients with newly diagnosed HER2-positive breast cancer.
Methods: We derived a combined prognostic model using retrospective clinical-pathological data on stromal tumour-infiltrating lymphocytes, PAM50 subtypes, and expression of 55 genes obtained from patients who participated in the Short-HER phase 3 trial. The trial enrolled patients with newly diagnosed, node-positive, HER2-positive breast cancer or, if node negative, with at least one risk factor (ie, tumour size >2 cm, histological grade 3, lymphovascular invasion, Ki67 >20%, age ≤35 years, or hormone receptor negativity), and randomly assigned them to adjuvant anthracycline plus taxane-based combinations with either 9 weeks or 1 year of trastuzumab. Trastuzumab was administered intravenously every 3 weeks (8 mg/kg loading dose at first cycle, and 6 mg/kg thereafter) for 18 doses or weekly (4 mg/kg loading dose in the first week, and 2 mg/kg thereafter) for 9 weeks, starting concomitantly with the first taxane dose. Median follow-up was 91·4 months (IQR 75·1-105·6). The primary objective of our study was to derive and evaluate a combined prognostic score associated with distant metastasis-free survival (the time between randomisation and distant recurrence or death before recurrence), an exploratory endpoint in Short-HER. Patient samples in the training dataset were split into a training set (n=290) and a testing set (n=145), balancing for event and treatment group. The training set was further stratified into 100 iterations of Monte-Carlo cross validation (MCCV). Cox proportional hazard models were fit to MCCV training samples using Elastic-Net. A maximum of 92 features were assessed. The final prognostic model was evaluated in an independent combined dataset of 267 patients with early-stage HER2-positive breast cancer treated with different neoadjuvant and adjuvant anti-HER2-based combinations and from four other studies (PAMELA, CHER-LOB, Hospital Clinic, and Padova) with disease-free survival outcome data.
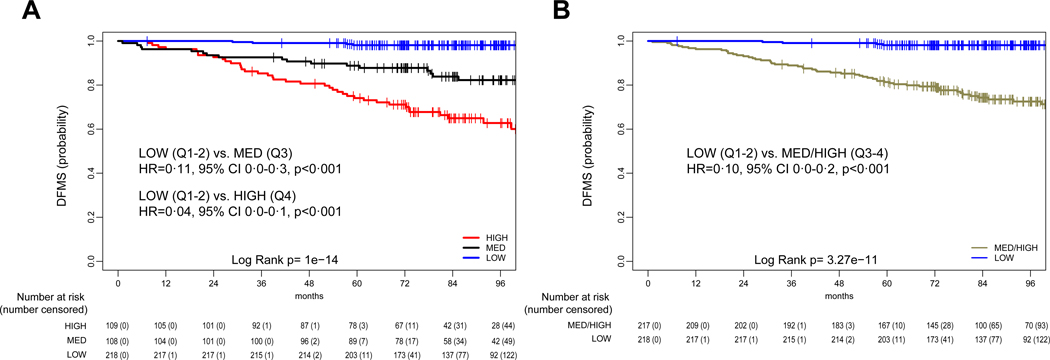
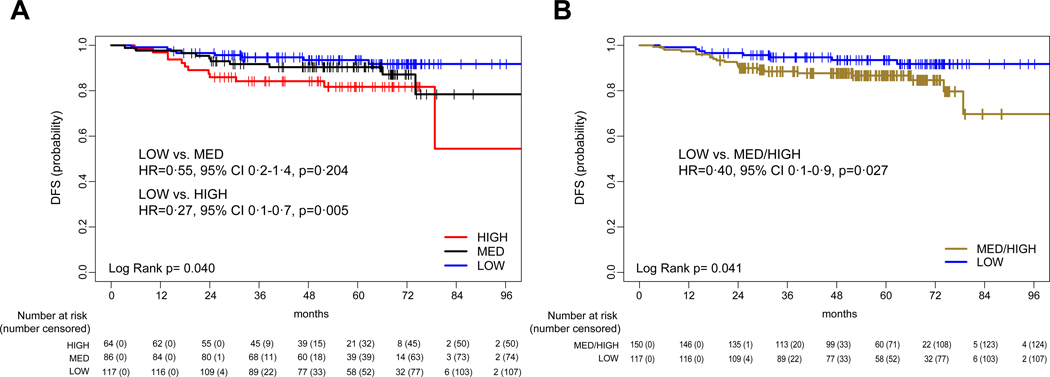
Findings: From Short-HER, data from 435 (35%) of 1254 patients for tumour size (T1 vs rest), nodal status (N0 vs rest), number of tumour-infiltrating lymphocytes (continuous variable), subtype (HER2-enriched and basal-like vs rest), and 13 genes composed the final model (named HER2DX). HER2DX was significantly associated with distant metastasis-free survival as a continuous variable (p<0·0001). HER2DX median score for quartiles 1-2 was identified as the cutoff to identify low-risk patients; and the score that distinguished quartile 3 from quartile 4 was the cutoff to distinguish medium-risk and high-risk populations. The 5-year distant metastasis-free survival of the low-risk, medium-risk, and high-risk populations were 98·1% (95% CI 96·3-99·9), 88·9% (83·2-95·0), and 73·9% (66·0-82·7), respectively (low-risk vs high-risk hazard ratio [HR] 0·04, 95% CI 0·0-0·1, p<0·0001). In the evaluation cohort, HER2DX was significantly associated with disease-free survival as a continuous variable (HR 2·77, 95% CI 1·4-5·6, p=0·0040) and as group categories (low-risk vs high-risk HR 0·27, 0·1-0·7, p=0·005). 5-year disease-free survival in the HER2DX low-risk group was 93·5% (89·0-98·3%) and in the high-risk group was 81·1% (71·5-92·1).
Interpretation: The HER2DX combined prognostic score identifies patients with early-stage, HER2-positive breast cancer who might be candidates for escalated or de-escalated systemic treatment. Future clinical validation of HER2DX seems warranted to establish its use in different scenarios, especially in the neoadjuvant setting.
Funding: Instituto Salud Carlos III, Save the Mama, Pas a Pas, Fundación Científica, Asociación Española Contra el Cáncer, Fundación SEOM, National Institutes of Health, Agenzia Italiana del Farmaco, International Agency for Research on Cancer, and the Veneto Institute of Oncology, and Italian Association for Cancer Research.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
HER2DX: a tool that might inform treatment choices for HER2-positive breast cancer.Lancet Oncol. 2020 Nov;21(11):1392-1393. doi: 10.1016/S1470-2045(20)30552-0. Lancet Oncol. 2020. PMID: 33152281 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
