

A new fluoroscopic view for evaluation of anteromedial cortex reduction quality during cephalomedullary nailing for intertrochanteric femur fractures: the 30° oblique tangential projection
- PMID: 33153440
- PMCID: PMC7643444
- DOI: 10.1186/s12891-020-03668-6
A new fluoroscopic view for evaluation of anteromedial cortex reduction quality during cephalomedullary nailing for intertrochanteric femur fractures: the 30° oblique tangential projection
Abstract
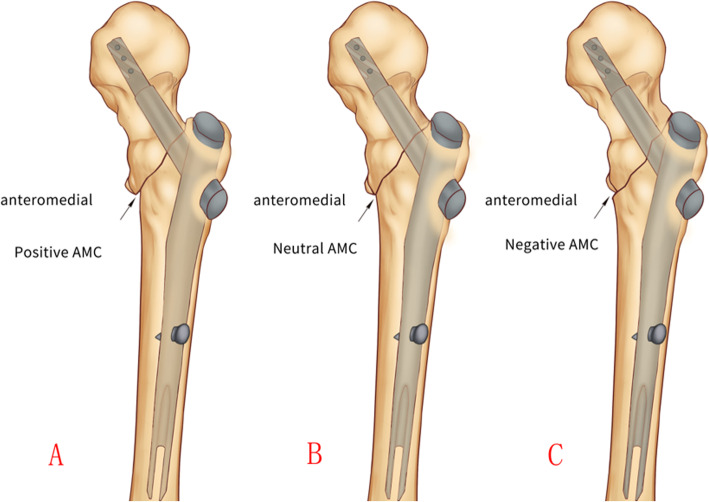
Background: Anteromedial cortex-to-cortex reduction is a key parameter for stable reconstruction of the fracture fragments during the intertrochanteric fracture fixation. This paper introduces the oblique fluoroscopic projection as a novel method to evaluate the quality of anteromedial cortical apposition.
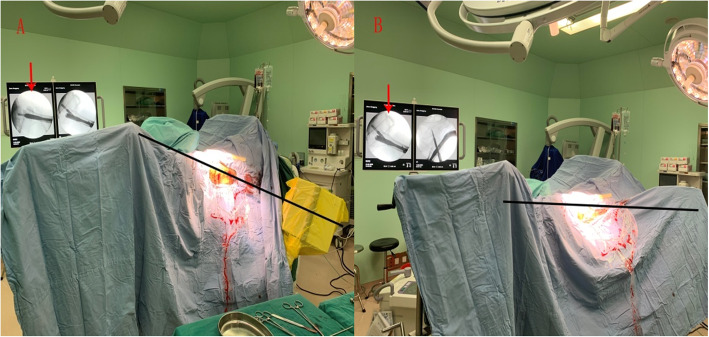
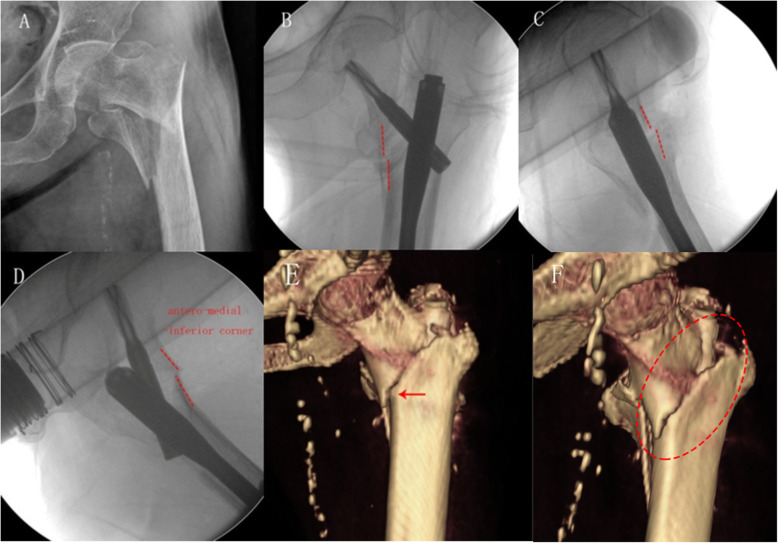
Methods: Three proximal femur specimens were marked with steel wires along five anatomic landmarks: Greater trochanter, Lesser trochanter, Intertrochanteric line, Anterolateral tubercle and the Anteromedial cortical line. After obtaining the standard femoral neck AP and lateral fluoroscopic images, the C-arm was rotated by every 5°increments until a clear tangential view of the antero-medial-inferior corner cortex was observed. 98 cases of intertrochanteric hip fractures were enrolled from April 2018 to October 2019. After fixation with the nails, the intra-operative anteromedial cortex reduction quality was evaluated from the AP, the true lateral, and the new anteromedial oblique fluoroscopic images. The fluoroscopic results were compared with the post-operative 3D-CT reconstruction images.
Results: The specimen study showed that internal rotation of the C-arm to approximately 30 ° can remove all the obscure shadows and clearly display the antero-medial-inferior cortical tangent line. Clinically,the positive, neutral and negative apposition of different cortices via intra-operative fluoroscopic images showed79, 19 and 0 cases of medial cortical apposition in AP views; 2, 68 and 28 cases of anterior cortices in lateral views;and 22, 51 and 25cases of anteromedial cortical apposition in oblique views respectively. The post-operative 3D-CT reconstruction images revealed that the final anteromedial cortical contact was noted in 62 cases (63.3%), and lost in 36 cases (36.7%). The overall coincidence rate between intra-operative fluoroscopy and post-operative 3D-CT was 63.3% (62/98) in AP view,79.6% (78/98) in lateral view, and 86.7% (85/98) in oblique view(p < 0.001). Negative cortical apposition in oblique view was highly predictive of a final loss of cortical support on 3D CT (24/25 cases, 96%).And non-negative cortical apposition in oblique view was highly associated with true cortical support on 3D CT images (61/73 cases, 83.6%) (p < 0.001).
Conclusions: Besides the AP and lateral projections, an anteromedial oblique view of 30° certifies to be a very useful means for evaluation of the fracture reduction quality of anteromedial cortical apposition.
Keywords: 3D-CT; Anteromedial cortex; Cortical apposition; Fluoroscopy; Oblique view; Pertrochanteric fracture.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

References
-
- Veronese N, Maggi S. Epidemiology and social costs of hip fracture. Injury. 2018;49:1458–1460. - PubMed
-
- Shannon SF, Yuan BJ, Cross WW, III, Barlow JD, Torchia ME, Holte PK, et al. Short versus long Cephalomedullary nails for Pertrochanteric hip fractures: a randomized prospective study. J Orthop Trauma. 2019;33(10):480–486. - PubMed
-
- Chang SM, Hou ZY, Hu SJ, Du SC. Intertrochanteric femur fracture treatment in Asia: what we know and what the world can learn. Orthopedic Clinics. 2020;51(2):189–205. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
