

Preventable medication harm across health care settings: a systematic review and meta-analysis
- PMID: 33153451
- PMCID: PMC7646069
- DOI: 10.1186/s12916-020-01774-9
Preventable medication harm across health care settings: a systematic review and meta-analysis
Abstract
Background: Mitigating or reducing the risk of medication harm is a global policy priority. But evidence reflecting preventable medication harm in medical care and the factors that derive this harm remain unknown. Therefore, we aimed to quantify the prevalence, severity and type of preventable medication harm across medical care settings.
Methods: We performed a systematic review and meta-analysis of observational studies to compare the prevalence of preventable medication harm. Searches were carried out in Medline, Cochrane library, CINAHL, Embase and PsycINFO from 2000 to 27 January 2020. Data extraction and critical appraisal was undertaken by two independent reviewers. Random-effects meta-analysis was employed followed by univariable and multivariable meta-regression. Heterogeneity was quantified using the I2 statistic, and publication bias was evaluated.
Prospero: CRD42020164156.
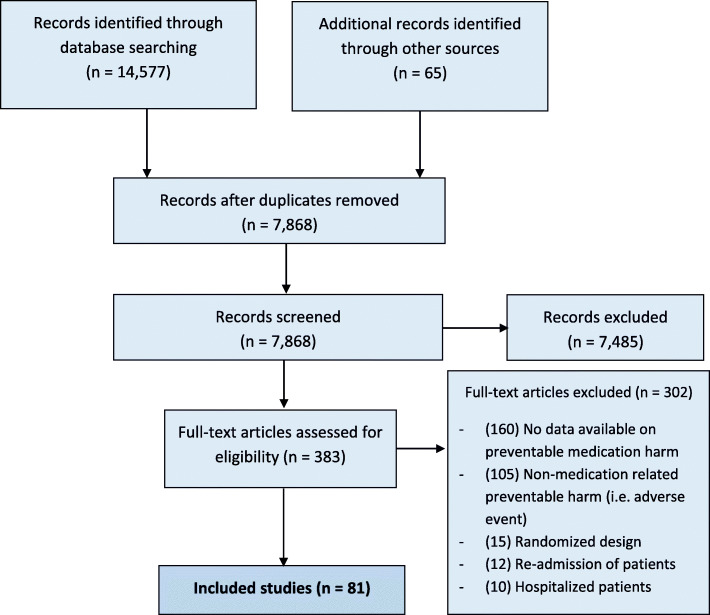
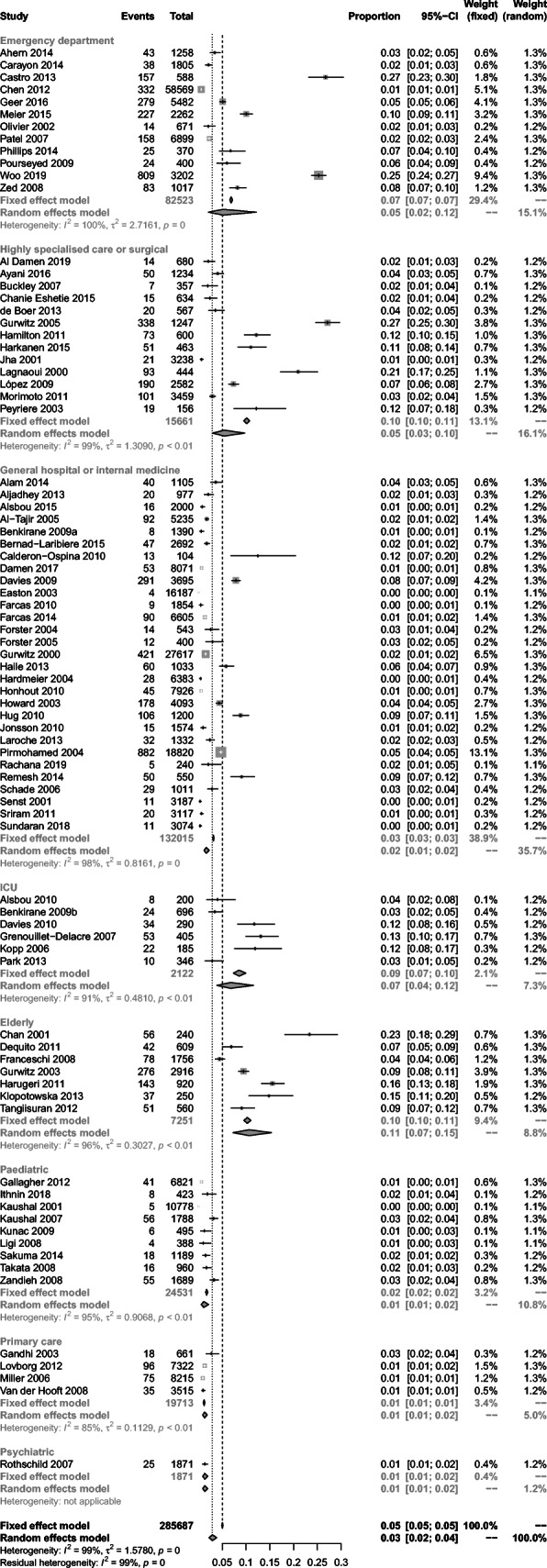
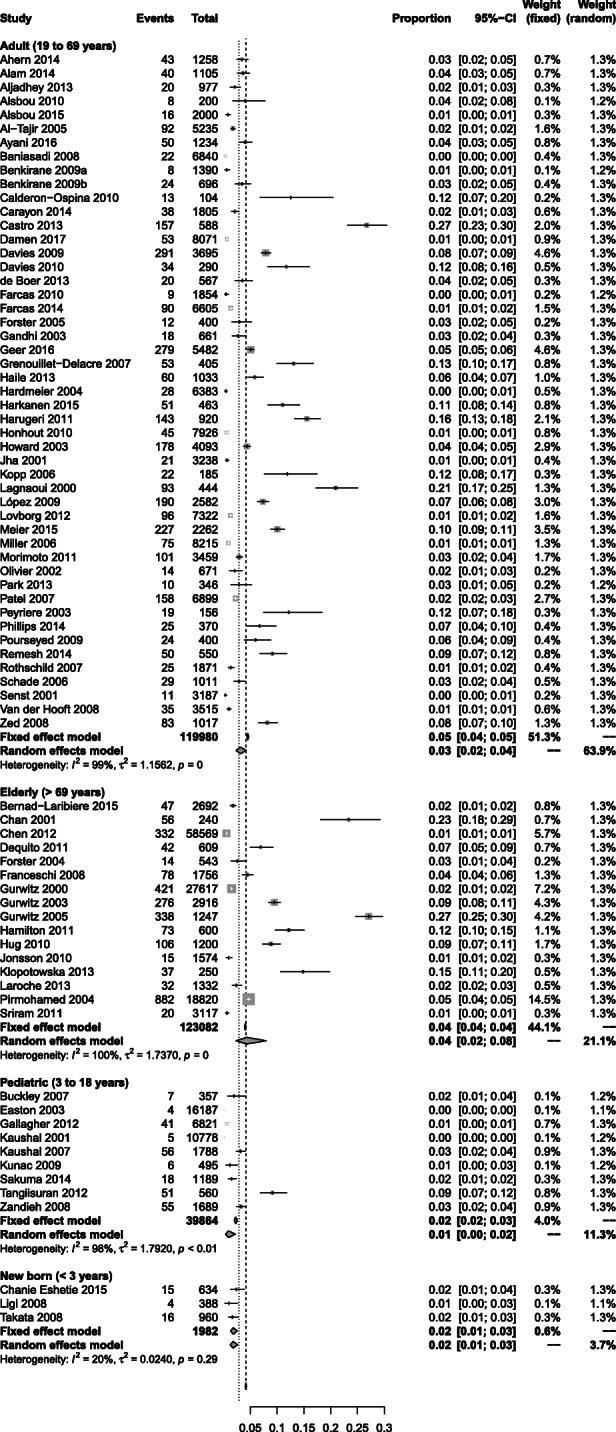
Results: Of the 7780 articles, 81 studies involving 285,687 patients were included. The pooled prevalence for preventable medication harm was 3% (95% confidence interval (CI) 2 to 4%, I2 = 99%) and for overall medication harm was 9% (95% CI 7 to 11%, I2 = 99.5%) of all patient incidence records. The highest rates of preventable medication harm were seen in elderly patient care settings (11%, 95% 7 to 15%, n = 7), intensive care (7%, 4 to 12%, n = 6), highly specialised or surgical care (6%, 3 to 11%, n = 13) and emergency medicine (5%, 2 to 12%, n = 12). The proportion of mild preventable medication harm was 39% (28 to 51%, n = 20, I2 = 96.4%), moderate preventable harm 40% (31 to 49%, n = 22, I2 = 93.6%) and clinically severe or life-threatening preventable harm 26% (15 to 37%, n = 28, I2 = 97%). The source of the highest prevalence rates of preventable harm were at the prescribing (58%, 42 to 73%, n = 9, I2 = 94%) and monitoring (47%, 21 to 73%, n = 8, I2 = 99%) stages of medication use. Preventable harm was greatest in medicines affecting the 'central nervous system' and 'cardiovascular system'.
Conclusions: This is the largest meta-analysis to assess preventable medication harm. We conclude that around one in 30 patients are exposed to preventable medication harm in medical care, and more than a quarter of this harm is considered severe or life-threatening. Our results support the World Health Organisation's push for the detection and mitigation of medication-related harm as being a top priority, whilst highlighting other key potential targets for remedial intervention that should be a priority focus for future research.
Keywords: Medication error; Meta-analysis; Patient safety; Prevalence; Preventable medication harm.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Context-specific technology-based solutions may reduce the risk of preventable medication harm across healthcare settings.Evid Based Nurs. 2022 Apr;25(2):70. doi: 10.1136/ebnurs-2020-103383. Epub 2021 Jul 26. Evid Based Nurs. 2022. PMID: 34312288 No abstract available.
References
-
- Donaldson MS. An Overview of To Err is Human: Re-emphasizing the Message of Patient Safety. In: Hughes RG, editor. Patient safety and quality: an evidence-based handbook for nurses. Rockville: Agency for Healthcare Research and Quality (US); 2008. - PubMed
-
- The third WHO Global Patient Safety Challenge: medication without harm. Patient safety. WHO. Last accessed on 10 Sept 2020. Available at: https://www.who.int/patientsafety/medication-safety/en/.
-
- Institute for Healthcare Improvement. National Steering Committee for Patient safety. A national strategy for reducing harm. Last accessed on 10 Sept 2020. Available at: http://www.ihi.org/Engage/Initiatives/National-Steering-Committee-Patien....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
