

Characterizing temporal genomic heterogeneity in pediatric low-grade gliomas
- PMID: 33153497
- PMCID: PMC7643477
- DOI: 10.1186/s40478-020-01054-w
Characterizing temporal genomic heterogeneity in pediatric low-grade gliomas
Abstract
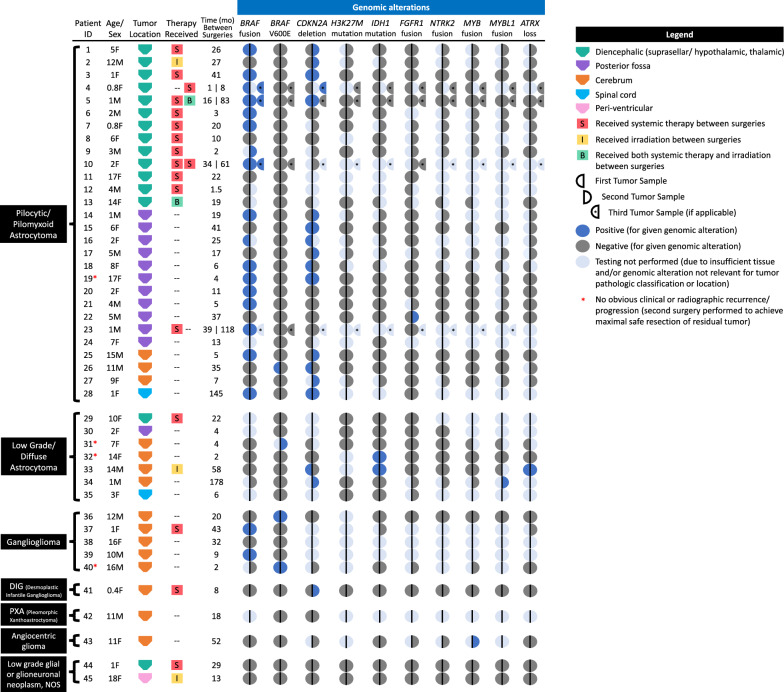
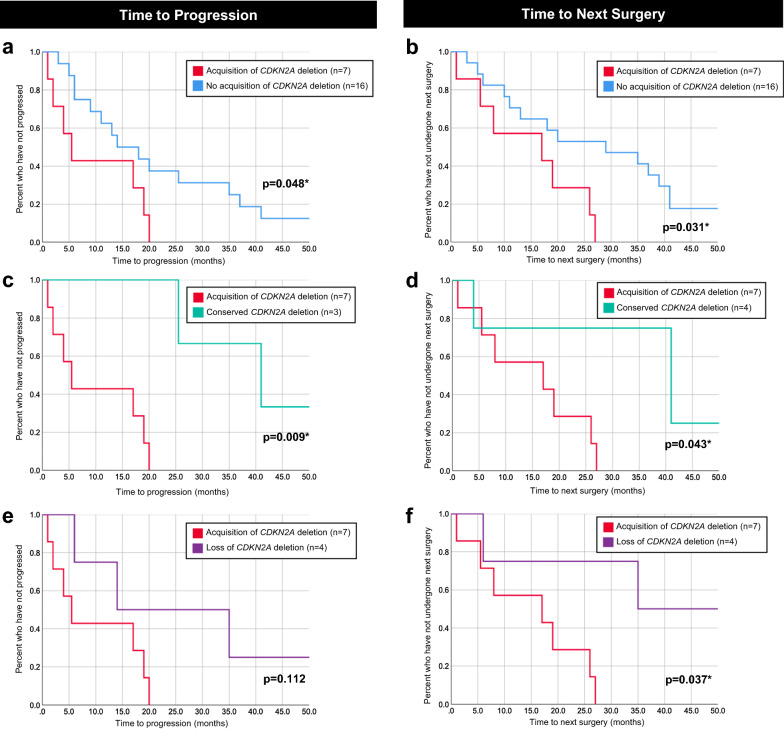
Recent discoveries have provided valuable insight into the genomic landscape of pediatric low-grade gliomas (LGGs) at diagnosis, facilitating molecularly targeted treatment. However, little is known about their temporal and therapy-related genomic heterogeneity. An adequate understanding of the evolution of pediatric LGGs' genomic profiles over time is critically important in guiding decisions about targeted therapeutics and diagnostic biopsy at recurrence. Fluorescence in situ hybridization, mutation-specific immunohistochemistry, and/or targeted sequencing were performed on paired tumor samples from primary diagnostic and subsequent surgeries. Ninety-four tumor samples from 45 patients (41 with two specimens, four with three specimens) from three institutions underwent testing. Conservation of BRAF fusion, BRAFV600E mutation, and FGFR1 rearrangement status was observed in 100%, 98%, and 96% of paired specimens, respectively. No loss or gain of IDH1 mutations or NTRK2, MYB, or MYBL1 rearrangements were detected over time. Histologic diagnosis remained the same in all tumors, with no acquired H3K27M mutations or malignant transformation. Changes in CDKN2A deletion status at recurrence occurred in 11 patients (42%), with acquisition of hemizygous CDKN2A deletion in seven and loss in four. Shorter time to progression and shorter time to subsequent surgery were observed among patients with acquired CDKN2A deletions compared to patients without acquisition of this alteration [median time to progression: 5.5 versus 16.0 months (p = 0.048); median time to next surgery: 17.0 months versus 29.0 months (p = 0.031)]. Most targetable genetic aberrations in pediatric LGGs, including BRAF alterations, are conserved at recurrence and following chemotherapy or irradiation. However, changes in CDKN2A deletion status over time were demonstrated. Acquisition of CDKN2A deletion may define a higher risk subgroup of pediatric LGGs with a poorer prognosis. Given the potential for targeted therapies for tumors harboring CDKN2A deletions, biopsy at recurrence may be indicated in certain patients, especially those with rapid progression.
Keywords: BRAF; CDKN2A; Genomics; Paired; Pediatric low-grade gliomas; Recurrence; Tumor evolution.
Figures
References
-
- (1988) A study of childhood brain tumors based on surgical biopsies from ten North American institutions: sample description. Childhood Brain Tumor Consortium. J Neurooncol 6:9–23. 10.1007/BF00163535 - PubMed
-
- Ater JL, Zhou T, Holmes E, Mazewski CM, Booth TN, Freyer DR, Lazarus KH, Packer RJ, Prados M, Sposto R, Vezina G, Wisoff JH, Pollack IF. Randomized study of two chemotherapy regimens for treatment of low-grade glioma in young children: a report from the Children’s Oncology Group. J Clin Oncol. 2012;30:2641–2647. doi: 10.1200/JCO.2011.36.6054. - DOI - PMC - PubMed
-
- Bandopadhayay P, Ramkissoon LA, Jain P, Bergthold G, Wala J, Zeid R, Schumacher SE, Urbanski L, O’Rourke R, Gibson WJ, Pelton K, Ramkissoon SH, Han HJ, Zhu Y, Choudhari N, Silva A, Boucher K, Henn RE, Kang YJ, Knoff D, Paolella BR, Gladden-Young A, Varlet P, Pages M, Horowitz PM, Federation A, Malkin H, Tracy AA, Seepo S, Ducar M, Van Hummelen P, Santi M, Buccoliero AM, Scagnet M, Bowers DC, Giannini C, Puget S, Hawkins C, Tabori U, Klekner A, Bognar L, Burger PC, Eberhart C, Rodriguez FJ, Hill DA, Mueller S, Haas-Kogan DA, Phillips JJ, Santagata S, Stiles CD, Bradner JE, Jabado N, Goren A, Grill J, Ligon AH, Goumnerova L, Waanders AJ, Storm PB, Kieran MW, Ligon KL, Beroukhim R, Resnick AC. MYB-QKI rearrangements in angiocentric glioma drive tumorigenicity through a tripartite mechanism. Nat Genet. 2016;48:273–282. doi: 10.1038/ng.3500. - DOI - PMC - PubMed
-
- Banerjee A, Jakacki RI, Onar-Thomas A, Wu S, Nicolaides T, Young Poussaint T, Fangusaro J, Phillips J, Perry A, Turner D, Prados M, Packer RJ, Qaddoumi I, Gururangan S, Pollack IF, Goldman S, Doyle LA, Stewart CF, Boyett JM, Kun LE, Fouladi M. A phase I trial of the MEK inhibitor selumetinib (AZD6244) in pediatric patients with recurrent or refractory low-grade glioma: a Pediatric Brain Tumor Consortium (PBTC) study. Neuro Oncol. 2017;19:1135–1144. doi: 10.1093/neuonc/now282. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
