

COVID-19 and COPD: a narrative review of the basic science and clinical outcomes
- PMID: 33153991
- PMCID: PMC7651840
- DOI: 10.1183/16000617.0199-2020
COVID-19 and COPD: a narrative review of the basic science and clinical outcomes
Abstract
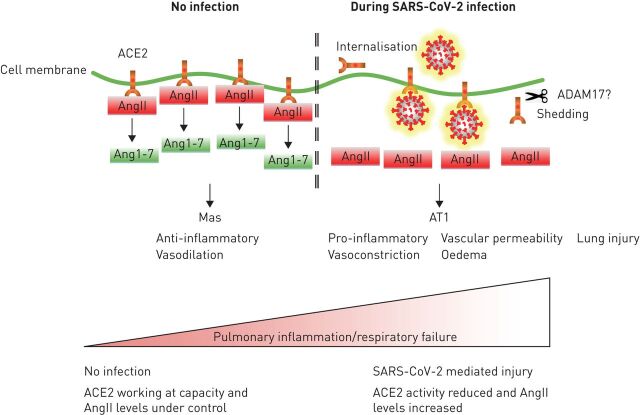
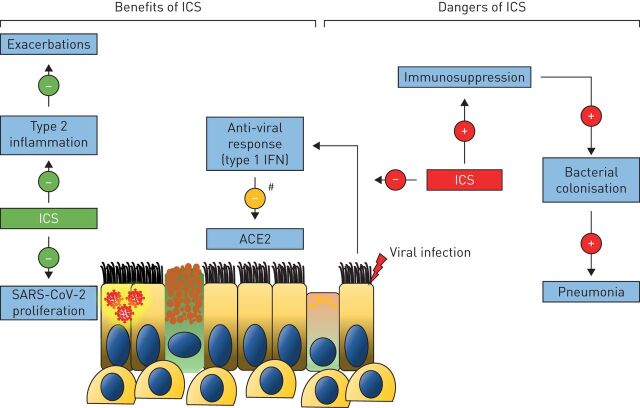
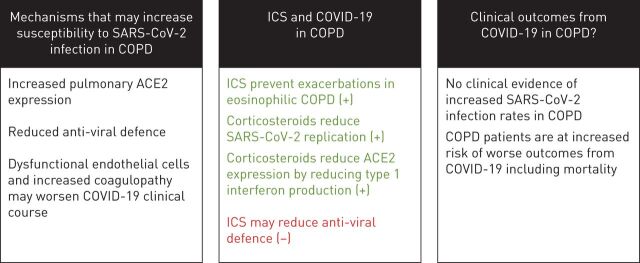
The 2019 coronavirus disease (COVID-19) pandemic is caused by severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2). Clinical outcomes, including mortality, are worse in males, older individuals and patients with comorbidities. COPD patients are included in shielding strategies due to their susceptibility to virus-induced exacerbations, compromised pulmonary function and high prevalence of associated comorbidities. Using evidence from basic science and cohort studies, this review addresses key questions concerning COVID-19 and COPD. First, are there mechanisms by which COPD patients are more susceptible to SARS-CoV-2 infection? Secondly, do inhaled corticosteroids offer protection against COVID-19? And, thirdly, what is the evidence regarding clinical outcomes from COVID-19 in COPD patients? This up-to-date review tackles some of the key issues which have significant impact on the long-term outlook for COPD patients in the context of COVID-19.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: A. Higham reports personal fees from Chiesi, outside the submitted work. Conflict of interest: A. Mathioudakis reports grants from Boehringer Ingelheim outside the submitted work. Conflict of interest: J. Vestbo reports personal fees from AstraZeneca, Boehringer-Ingelheim, Chiesi, GSK and Novartis, and grants from Boehringer-Ingelheim, outside the submitted work. Conflict of interest: D. Singh reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Genentech, GlaxoSmithKline, Glenmark, Gossamerbio, Menarini, Mundipharma, Novartis, Peptinnovate, Pfizer, Pulmatrix, Theravance and Verona, outside the submitted work.
Figures
References
-
- Centre for Health Protection of the Hong Kong Special Administrative Region Government . CHP closely monitors cluster of pneumonia cases on Mainland. www.info.gov.hk/gia/general/201912/31/P2019123100667.htm Date last updated: 31 December 2019; date last accessed: 12 June 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous