

Correlation of surgeon radiology assessment with laparoscopic disease site scoring in patients with advanced ovarian cancer
- PMID: 33154095
- PMCID: PMC8266398
- DOI: 10.1136/ijgc-2020-001718
Correlation of surgeon radiology assessment with laparoscopic disease site scoring in patients with advanced ovarian cancer
Abstract
Background: Radiographic triage measures in patients with new advanced ovarian cancer have yielded inconsistent results.
Objective: To determine the correlation between surgeon radiology assessment and laparoscopic scoring by disease sites in patients with newly diagnosed advanced stage ovarian cancer.
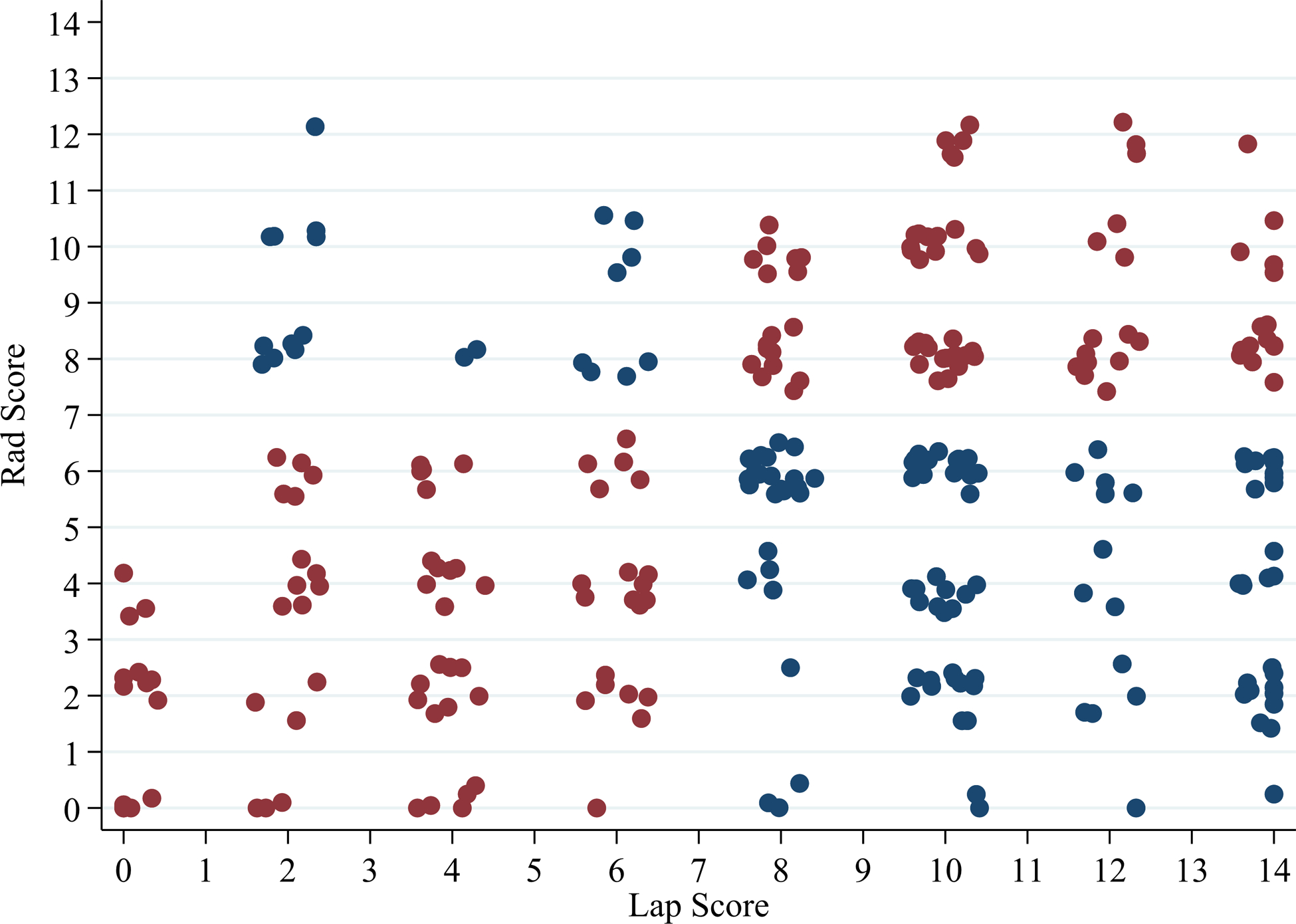
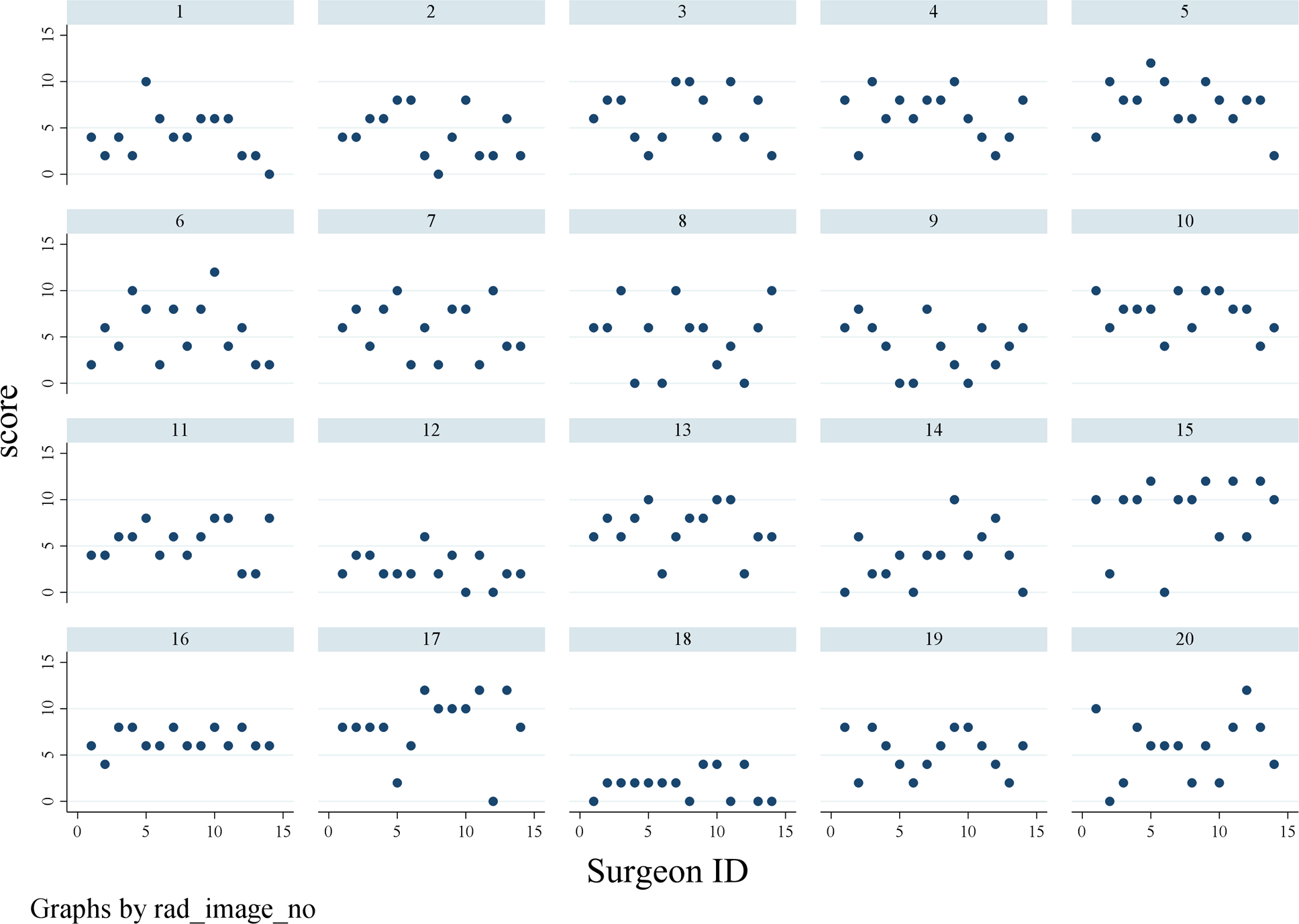
Methods: Fourteen gynecologic oncology surgeons from a single institution performed a blinded review of pre-operative contrast-enhanced CT imaging from patients with advanced stage ovarian cancer. Each of the patients had also undergone laparoscopic scoring assessment, between April 2013 and December 2017, to determine primary resectability using the validated Fagotti scoring method, and assigned a predictive index value score. Surgeons were asked to provide expected predictive index value scores based on their blinded review of the antecedent CT imaging. Linear mixed models were conducted to calculate the correlation between radiologic and laparoscopic score for surgeons individually, and as a group. Once the model was fit, the inter-class correlation and 95% CI were calculated.
Results: Radiology review was performed on 20 patients with advanced stage ovarian cancer who underwent laparoscopic scoring assessment. Surgeon faculty rank included assistant professor (n=5), associate professor (p=4), and professor (n=5). The kappa inter-rater agreement was -0.017 (95% CI -0.023 to -0.005), indicating low inter-rater agreement between radiology review and actual laparoscopic score. The inter-class correlation in this model was 0.06 (0.02-0.21), indicating that surgeons do not score the same across all the images. When using a clinical cut-off point for the predictive index value of 8, the probability of agreement between radiology and actual laparoscopic score was 0.56 (95% CI 0.49 to 0.73). Examination of disease site sub-scales showed that the probability of agreement was as follows: peritoneum 0.57 (95% CI 0.51 to 0.62), diaphragm 0.54 (95% CI 0.48 to 0.60), mesentery 0.51 (95% CI 0.45 to 0.57), omentum 0.61 (95% CI 0.55 to 0.67), bowel 0.54 (95% CI 0.44 to 0.64), stomach 0.71 (95% CI 0.65 to 0.76), and liver 0.36 (95% CI 0.31 to 0.42). The number of laparoscopic scoring cases, tumor reductive surgery cases, or faculty rank was not significantly associated with overall or sub-scale agreement.
Conclusions: Surgeon radiology review did not correlate highly with actual laparoscopic scoring assessment findings in patients with advanced stage ovarian cancer. Our study highlights the limited accuracy of surgeon radiographic assessment to determine resectability.
Keywords: cytoreduction surgical procedures; laparoscopes; ovarian cancer.
© IGCS and ESGO 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: The authors have the following conflicts of interest to disclosure. Relevant financial activities outside the supported work; NDF: consultant/advisory board (Tesaro, BMS/Pfizer); SNW: consultant (AstraZeneca, Clovis Oncology, GSK/Tesaro, Novartis, Roche/Genentech, Eisai, Merck, Pfizer, Circulogene), research funding (ArQule, AstraZeneca, Clovis Oncology, GSK/Tesaro, Novartis, Roche/Genentech, Bayer, Cotinga Pharmaceuticals); LAM: research funding (AstraZeneca); AJ: consultant (Gerson and Lehrman Group, Guidepoint, Iovance, Nuprobe, Simcere, Pact Pharma), research funding (AstraZeneca, BMS, Iovance, Aravive, Pfizer, Immatics USA, Eli Lilly); RLC: consultant (AstraZeneca, Clovis Oncology, GSK/Tesaro, Novartis, Roche/Genentech, Eisai, Merck, Pfizer, Novocure, Genmab, Gamamab, Oncosec, Tarveda), research funding (AbbVie, Genmab, Merck, AstraZeneca, Clovis Oncology, Roche/Genentech); AKS: consultant (Merck, Kiyatec), shareholder (Biopath), research funding (M-Trap). The following authors have no disclosures: PB, JAR-H, PS, AS, MO, LC, MB, BMF, JB, BZ, CL.
Figures
References
-
- Axtell AE, Lee MH, Bristow RE, et al. Multi-institutional reciprocal validation study of computed tomography predictors of suboptimal primary cytoreduction in patients with advanced ovarian cancer. J Clin Oncol 2007;25:384–9. - PubMed
-
- Suidan RS, Ramirez PT, Sarasohn DM, et al. A multicenter prospective trial evaluating the ability of preoperative computed tomography scan and serum CA-125 to predict suboptimal cytoreduction at primary debulking surgery for advanced ovarian, fallopian tube, and peritoneal cancer. Gynecol Oncol 2014;134:455–61. - PMC - PubMed
-
- Aletti GD, Eisenhauer EL, Santillan A, et al. Identification of patient groups at highest risk from traditional approach to ovarian cancer treatment. Gynecol Oncol 2011;120:23–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
