

Multilevel modelling and multiple group analysis of disparities in continuity of care and viral suppression among adolescents and youths living with HIV in Nigeria
- PMID: 33154102
- PMCID: PMC7646327
- DOI: 10.1136/bmjgh-2020-003269
Multilevel modelling and multiple group analysis of disparities in continuity of care and viral suppression among adolescents and youths living with HIV in Nigeria
Abstract
Introduction: Substantial disparities in care outcomes exist between different subgroups of adolescents and youths living with HIV (AYLHIV). Understanding variation in individual and health facility characteristics could be key to identifying targets for interventions to reduce these disparities. We modelled variation in AYLHIV retention in care and viral suppression, and quantified the extent to which individual and facility characteristics account for observed variations.
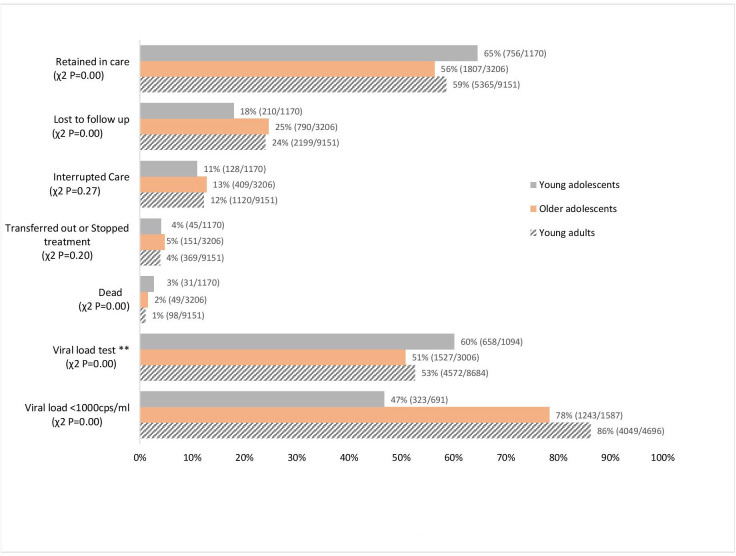
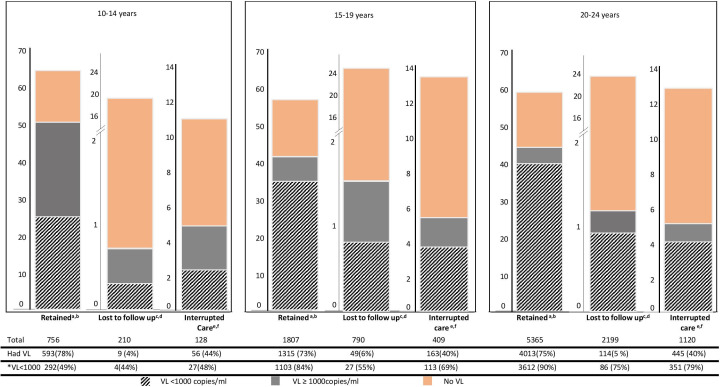
Methods: We included 1170 young adolescents (10-14 years), 3206 older adolescents (15-19 years) and 9151 young adults (20-24 years) who were initiated on antiretroviral therapy (ART) between January 2015 and December 2017 across 124 healthcare facilities in Nigeria. For each age group, we used multilevel modelling to partition observed variation of main outcomes (retention in care and viral suppression at 12 months after ART initiation) by individual (level one) and health facility (level two) characteristics. We used multiple group analysis to compare the effects of individual and facility characteristics across age groups.
Results: Facility characteristics explained most of the observed variance in retention in care in all the age groups, with smaller contributions from individual-level characteristics (14%-22.22% vs 0%-3.84%). For viral suppression, facility characteristics accounted for a higher proportion of variance in young adolescents (15.79%), but not in older adolescents (0%) and young adults (3.45%). Males were more likely to not be retained in care (adjusted OR (aOR)=1.28; p<0.001 young adults) and less likely to achieve viral suppression (aOR=0.69; p<0.05 older adolescent). Increasing facility-level viral load testing reduced the likelihood of non-retention in care, while baseline regimen TDF/3TC/EFV or NVP increased the likelihood of viral suppression.
Conclusions: Differences in characteristics of healthcare facilities accounted for observed disparities in retention in care and, to a lesser extent, disparities in viral suppression. An optimal combination of individual and health services approaches is, therefore, necessary to reduce disparities in the health and well-being of AYLHIV.
Keywords: HIV; health services research; public health.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- WHO UNAIDS update: active involvement of young people is key to ending the AIDS epidemic by 2030, 2017.
-
- Said M, Bartlett AW. Immune dysfunction and antiretroviral therapy challenges in children and adolescents living with human immunodeficiency virus. Innate Immun Health Dis 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical