

Deep learning-based model for detecting 2019 novel coronavirus pneumonia on high-resolution computed tomography
- PMID: 33154542
- PMCID: PMC7645624
- DOI: 10.1038/s41598-020-76282-0
Deep learning-based model for detecting 2019 novel coronavirus pneumonia on high-resolution computed tomography
Abstract
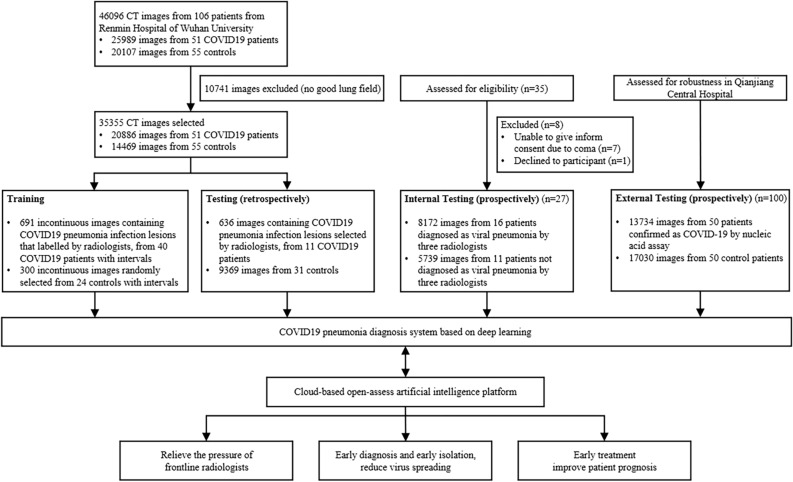
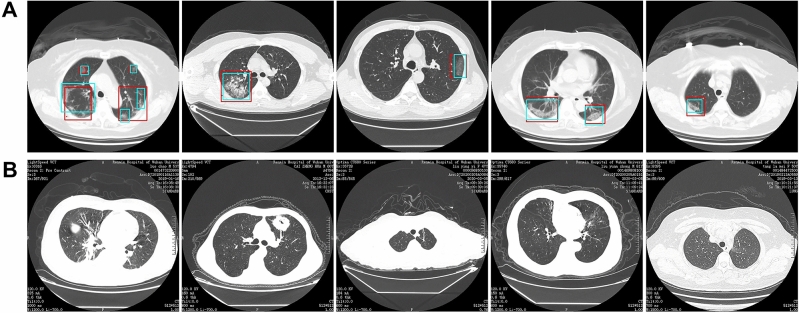
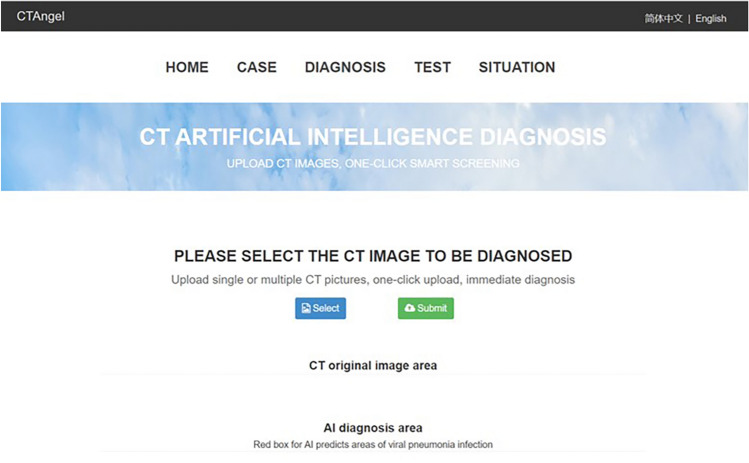
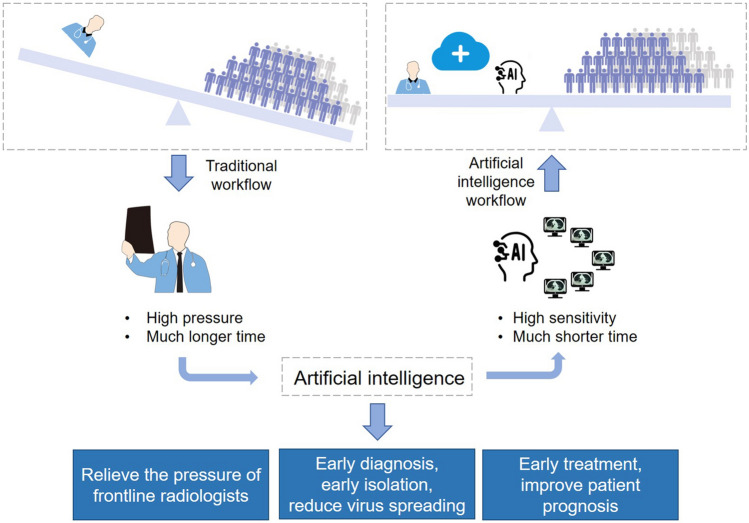
Computed tomography (CT) is the preferred imaging method for diagnosing 2019 novel coronavirus (COVID19) pneumonia. We aimed to construct a system based on deep learning for detecting COVID-19 pneumonia on high resolution CT. For model development and validation, 46,096 anonymous images from 106 admitted patients, including 51 patients of laboratory confirmed COVID-19 pneumonia and 55 control patients of other diseases in Renmin Hospital of Wuhan University were retrospectively collected. Twenty-seven prospective consecutive patients in Renmin Hospital of Wuhan University were collected to evaluate the efficiency of radiologists against 2019-CoV pneumonia with that of the model. An external test was conducted in Qianjiang Central Hospital to estimate the system's robustness. The model achieved a per-patient accuracy of 95.24% and a per-image accuracy of 98.85% in internal retrospective dataset. For 27 internal prospective patients, the system achieved a comparable performance to that of expert radiologist. In external dataset, it achieved an accuracy of 96%. With the assistance of the model, the reading time of radiologists was greatly decreased by 65%. The deep learning model showed a comparable performance with expert radiologist, and greatly improved the efficiency of radiologists in clinical practice.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Guan H, et al. Clinical and thin-section CT features of patients with the COVID-19 in Wuhan (in Chinese) Radiol. Pract. 2020;35:125–130.
