

Aortopulmonary window: Types, associated cardiovascular anomalies, and surgical outcome. Retrospective analysis of a single center experience
- PMID: 33154906
- PMCID: PMC7640542
- DOI: 10.37616/2212-5043.20
Aortopulmonary window: Types, associated cardiovascular anomalies, and surgical outcome. Retrospective analysis of a single center experience
Abstract
Objective: Aortopulmonary window (APW) is a rare congenital heart defect. It occurs as an isolated cardiac lesion or in association with other cardiac anomalies and rarely with abnormal coronary arteries. The spectrum of cardiovascular anomalies associated with APW and overall management and outcome in the current era were reviewed.
Methods: Between 2001 and 2018, all patients diagnosed with APW were included. Based on associated cardiovascular anomalies, those patients were divided into 2 groups: simple APW group and complex APW group (APW with associated other cardiovascular anomalies). All cases were followed longitudinally. The outcomes are described.
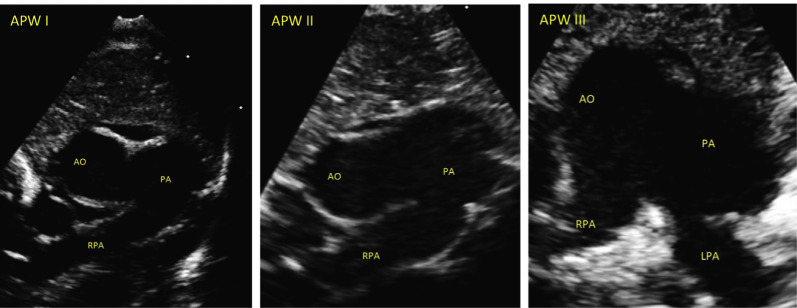
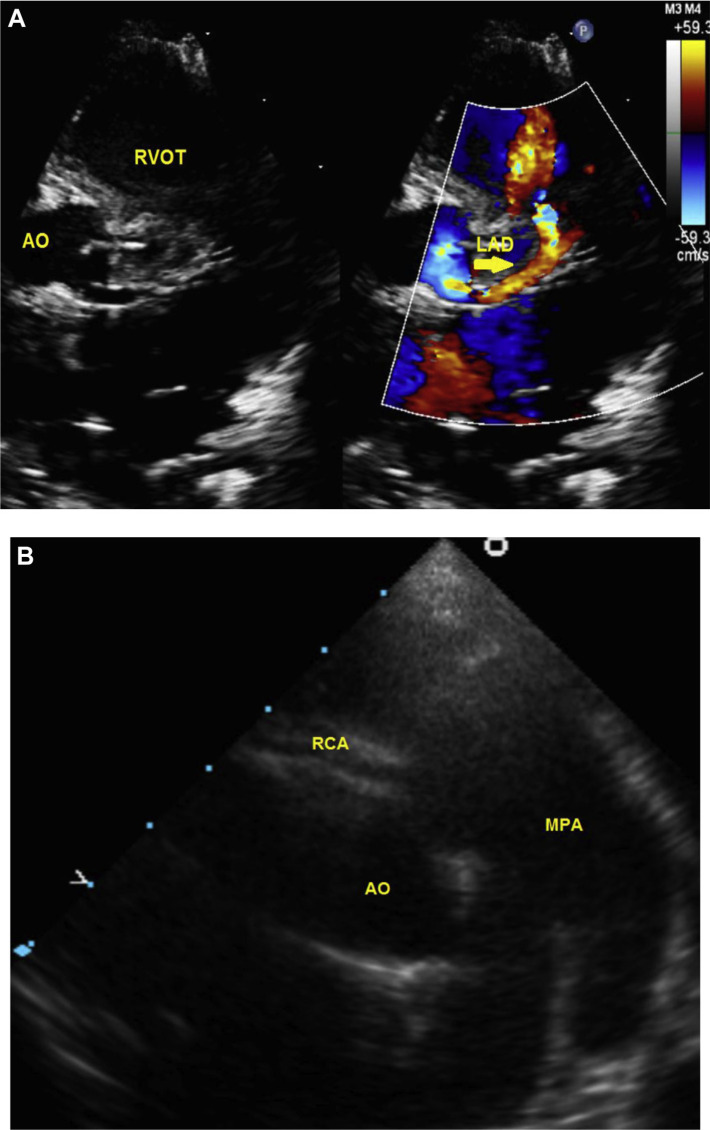
Result: Twenty patients underwent APW repair including 2 (10%) in simple APW group and 18 (90%) in complex APW group. Their mean age and weight were 4.8 ± 1.8 months and 4 ± 0.4 kg, respectively. APW Type I was confirmed in 65% followed by Type III in 20% and then Type II in 15% of the patients. In the complex APW group, atrial septal defect was the commonest associated cardiac lesion occurring in 8/20 (40%), followed by ventricular septal defect, interrupted aortic arch, and pulmonary artery anomalies in 25% of each. The presence of patent ductus arteriosus (PDA) was found in 40% of APW cases with 2/3rd of them in association with interrupted aortic arch. Two patients (10%) had unusual coronary anomalies that required repair, both with APW Type I. Associated non-cardiac anomalies were found in 30% of cases. Risk Adjustment for Congenital Heart Surgery (RACHS-1) score frequencies were between 2 and 4. Only one patient had reactive pulmonary hypertension related to chronic lung disease. All patients underwent surgical correction with median age of 2 month at the time of repair (interquartile range, 2 weeks to 4.5 months). Mean duration of mechanical ventilation, pediatric cardiac ICU and hospital length of stay were 2.8 ± 0.5, 9 ± 3 and 26 ± 6 days, respectively. All patients survived with no residual APW with mean follow-up duration of 4.5 years.
Conclusion: Majority of APW are associated with other cardiovascular anomalies (90%) including coronary abnormalities (10%). Early surgical repair of APW and associated lesions showed excellent survival rate, freedom from re-intervention need within an average of 4.5 years of follow up and no evidence of persistent pulmonary hypertension post repair.
Keywords: Aortopulmonary window; Cardiovascular anomalies; Pediatric cardiac surgery.
© 2020 Saudi Heart Association.
Conflict of interest statement
The authors have no conflicts of interest relevant to this article.
Figures
Similar articles
-
Current Outcomes of Surgical Management of Aortopulmonary Window and Associated Cardiac Lesions.Ann Thorac Surg. 2016 Aug;102(2):608-14. doi: 10.1016/j.athoracsur.2016.02.035. Epub 2016 May 18. Ann Thorac Surg. 2016. PMID: 27207392
-
Operative Repair of Aortopulmonary Window: A 25-Year Experience.World J Pediatr Congenit Heart Surg. 2024 Jul;15(4):472-480. doi: 10.1177/21501351241235959. Epub 2024 Apr 22. World J Pediatr Congenit Heart Surg. 2024. PMID: 38646828
-
Surgical outcome of aortopulmonary window repair in early infancy.J Formos Med Assoc. 2006 Oct;105(10):813-20. doi: 10.1016/S0929-6646(09)60268-0. J Formos Med Assoc. 2006. PMID: 17000454
-
Aortopulmonary window associated with interrupted aortic arch: report of surgical repair of eight cases and review of literature.Thorac Cardiovasc Surg. 2012 Apr;60(3):215-20. doi: 10.1055/s-0031-1298061. Epub 2012 Jan 17. Thorac Cardiovasc Surg. 2012. PMID: 22252330 Review.
-
Outcomes in patients with interrupted aortic arch and associated anomalies: a 20-year experience.Eur J Cardiothorac Surg. 2006 May;29(5):666-73; discussion 673-4. doi: 10.1016/j.ejcts.2006.01.060. Epub 2006 Apr 12. Eur J Cardiothorac Surg. 2006. PMID: 16626964 Review.
Cited by
-
Late Identification of a Stealthy Aorto-Pulmonary Window: A Case Report.Cureus. 2023 Jul 27;15(7):e42524. doi: 10.7759/cureus.42524. eCollection 2023 Jul. Cureus. 2023. PMID: 37637538 Free PMC article.
-
Berry syndrome; a successful one-stage repair in neonate periods, evaluation result after 9 years, a case report.Ann Med Surg (Lond). 2021 Mar 4;64:102200. doi: 10.1016/j.amsu.2021.102200. eCollection 2021 Apr. Ann Med Surg (Lond). 2021. PMID: 33732452 Free PMC article.
References
-
- Richardson JV, Doty DB, Rossi NP, Ehrenhaft JL. The spectrum of anomalies of aortopulmonary septation. J Thorac Cardiovasc Surg. 1979;78:21–7. - PubMed
-
- Zhu C, Wang T, Zhu Z, Liu K. Aberrant origin of left subclavian artery from the pulmonary artery and right aortic arch in an aortopulmonary window. Interact Cardiovasc Thorac Surg. 2016;23:991–2. - PubMed
LinkOut - more resources
Full Text Sources