

Staged surgical treatment of open Lisfranc fracture dislocations using an adjustable bilateral external fixator: A retrospective review of 21 patients
- PMID: 33155557
- PMCID: PMC7646616
- DOI: 10.5152/j.aott.2020.19221
Staged surgical treatment of open Lisfranc fracture dislocations using an adjustable bilateral external fixator: A retrospective review of 21 patients
Abstract
Objective: The aim of this study was to assess the early operative results of a staged progressive reduction technique using a bilateral external fixator in the treatment of patients with open Lisfranc fracture dislocations.
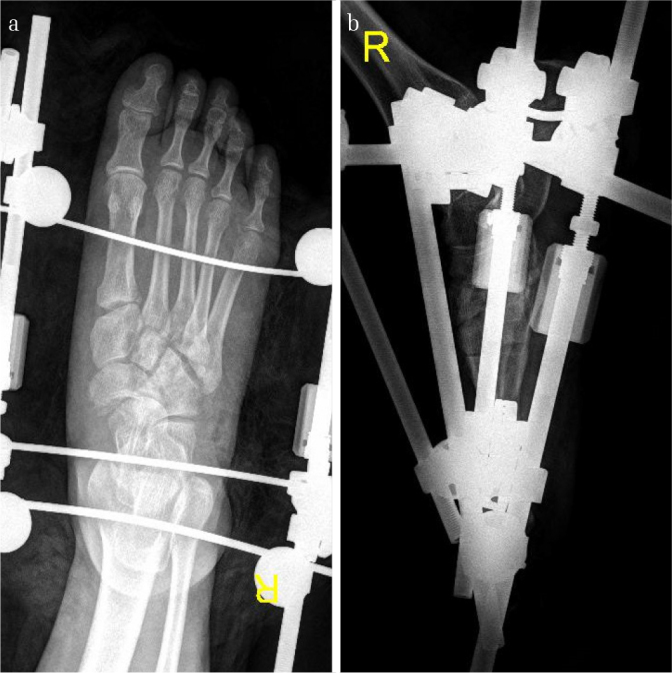
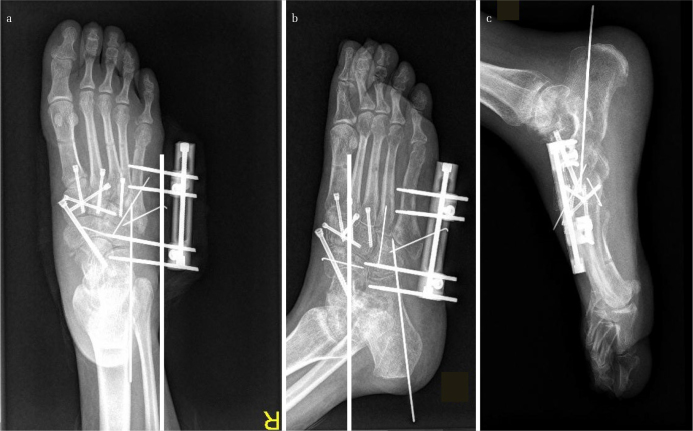
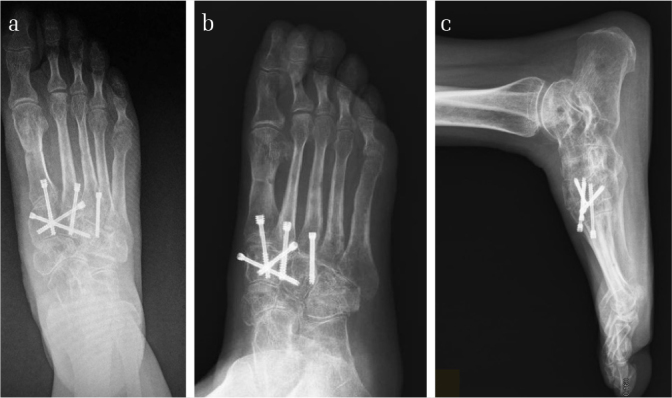
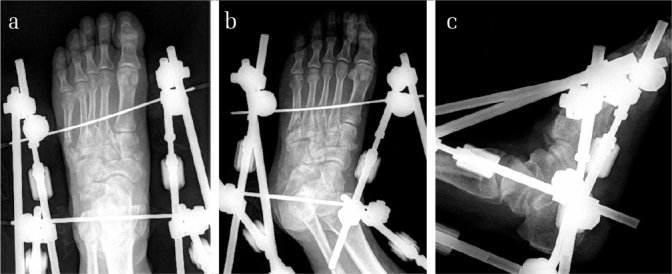
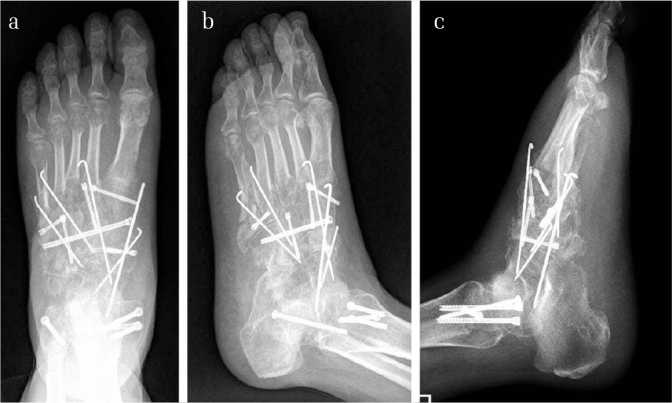
Methods: In this retrospective study, 21 patients (5 women and 16 men; mean age=44.4 years; age range=24 to 69 years) with open Lisfranc fracture dislocations were included. All the patients were treated in a staged manner from 2012 to 2015. The mean follow-up was 15.4 months (range=12 to 24 months). A two-stage surgical protocol was performed for each patient. At the first stage, a bilateral spanning external fixator was applied across the injured Lisfranc joint, and the length of the disrupted columns was restored by distraction process. Vacuum-assisted closure was used if required. At the second stage, the external fixator was removed, and open reduction and internal fixation were carried out. The time interval between the first and second stages and postoperative complications were documented. To assess the functional status of the patients, the visual analog scale (VAS) and the American Orthopaedic Foot - Ankle Society (AOFAS) midfoot scale were measured at the final follow-up. Radiographic parameters indicating the alignment of the midfoot after the second operation were examined.
Results: Deep infection in one patient and superficial infection in 2 patients were observed. Venous thrombosis was detected in 3 patients. The mean interval between the first and second stages was 18.6 days (range=8 to 48 days). The first metatarso-cuneiform step-off (p=0.002) and the second metatarso-cuneiform step-off (p=0.000) significantly improved at the final follow-up. The mean VAS score was 2.4 (range=0-5), and the mean AOFAS score was 76.3 (range=63 to 97). Primary arthrodesis was performed in seven patients, and six of the remaining 14 patients developed post-traumatic arthritis.
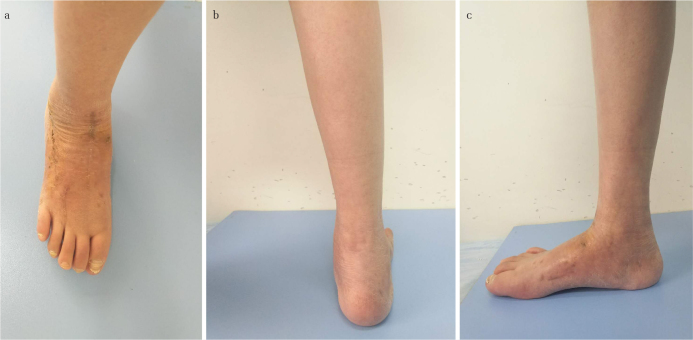
Conclusion: With a low risk of complications, the staged progressive reduction protocol using an adjustable bilateral external fixator can be an effective treatment to achieve and maintain anatomic reduction for patients with open Lisfranc fracture dislocations in a short-time follow-up.
Level of evidence: Level IV, Therapeutic study.
Conflict of interest statement
Figures





Similar articles
-
Long-term results of staged management of complex lisfranc and chopart injury: a retrospective cohort study and systematic literature review.Eur J Trauma Emerg Surg. 2025 Jan 24;51(1):49. doi: 10.1007/s00068-024-02747-w. Eur J Trauma Emerg Surg. 2025. PMID: 39853401 Free PMC article.
-
[Clinical and radiographic evaluation of open reduction and internal fixation with headless compression screws in treatment of lisfranc joint injuries].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013 Oct;27(10):1196-201. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013. PMID: 24397130 Chinese.
-
Temporary Bridge Plating vs Primary Arthrodesis of the First Tarsometatarsal Joint in Lisfranc Injuries: Randomized Controlled Trial.Foot Ankle Int. 2020 Aug;41(8):901-910. doi: 10.1177/1071100720925815. Epub 2020 Jun 5. Foot Ankle Int. 2020. PMID: 32501109 Free PMC article. Clinical Trial.
-
Staged Management of Missed Lisfranc Injuries: A Report of Short-term Results.Orthop Surg. 2017 Feb;9(1):54-61. doi: 10.1111/os.12320. Orthop Surg. 2017. PMID: 28371497 Free PMC article.
-
Open Reduction and Internal Fixation Versus Primary Arthrodesis for the Treatment of Acute Lisfranc Injuries: A Systematic Review and Meta-analysis.J Foot Ankle Surg. 2019 Mar;58(2):328-332. doi: 10.1053/j.jfas.2018.08.061. J Foot Ankle Surg. 2019. PMID: 30850102
Cited by
-
Long-term results of staged management of complex lisfranc and chopart injury: a retrospective cohort study and systematic literature review.Eur J Trauma Emerg Surg. 2025 Jan 24;51(1):49. doi: 10.1007/s00068-024-02747-w. Eur J Trauma Emerg Surg. 2025. PMID: 39853401 Free PMC article.
References
-
- Schepers T, Rammelt S. Classifying the Lisfranc injury: Literature overview and a new classification. FussSprungg. 2018;16:151–9. doi: 10.1016/j.fuspru.2018.07.003. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
