

Phenotypic clustering of dilated cardiomyopathy patients highlights important pathophysiological differences
- PMID: 33156912
- PMCID: PMC7813623
- DOI: 10.1093/eurheartj/ehaa841
Phenotypic clustering of dilated cardiomyopathy patients highlights important pathophysiological differences
Abstract
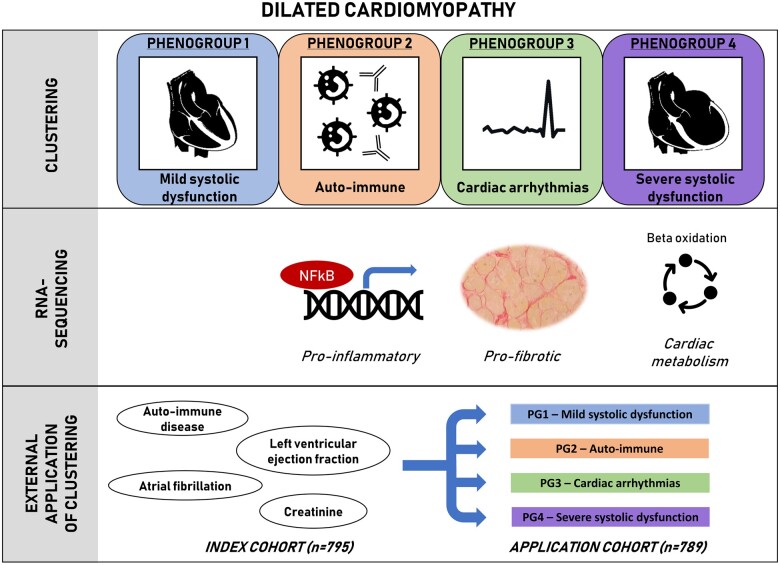
Aims: The dilated cardiomyopathy (DCM) phenotype is the result of combined genetic and acquired triggers. Until now, clinical decision-making in DCM has mainly been based on ejection fraction (EF) and NYHA classification, not considering the DCM heterogenicity. The present study aimed to identify patient subgroups by phenotypic clustering integrating aetiologies, comorbidities, and cardiac function along cardiac transcript levels, to unveil pathophysiological differences between DCM subgroups.
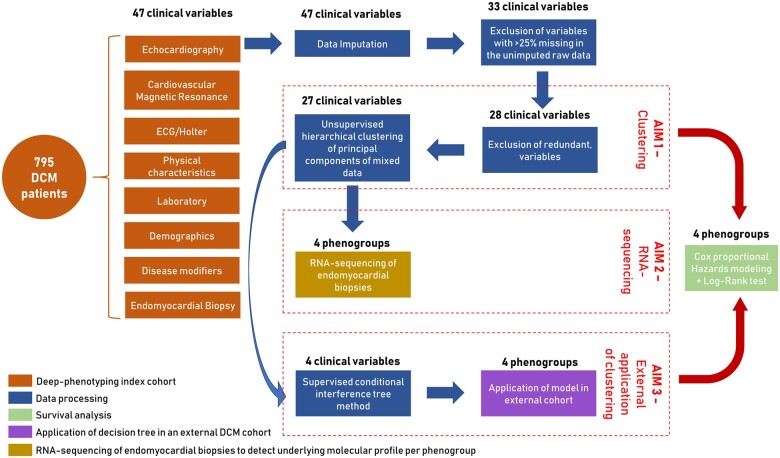
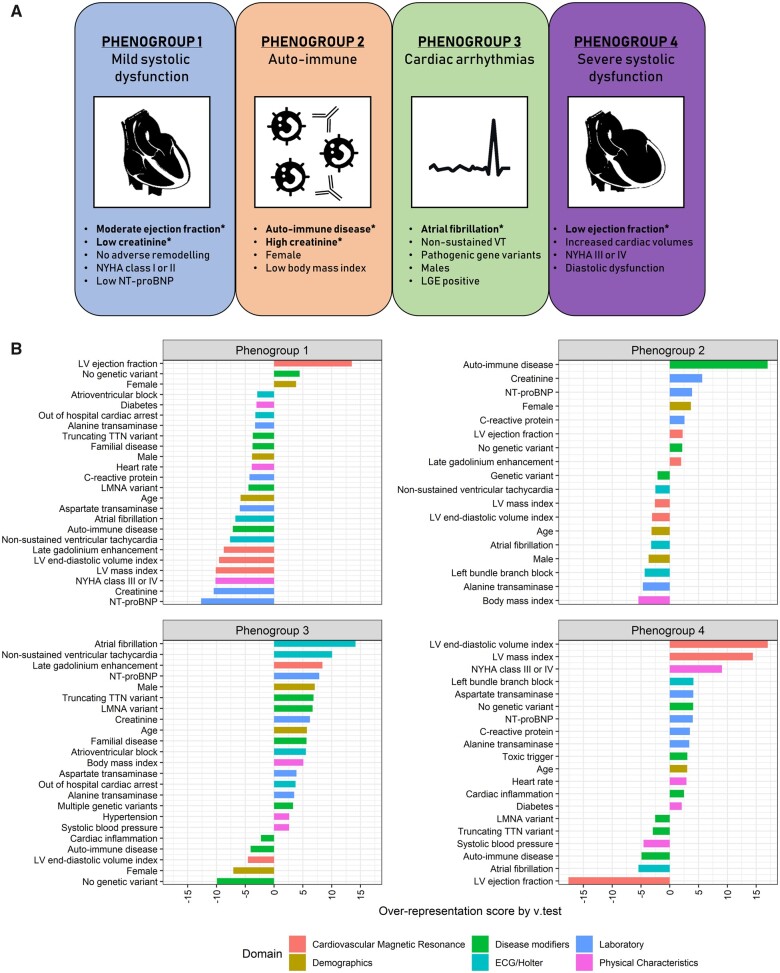
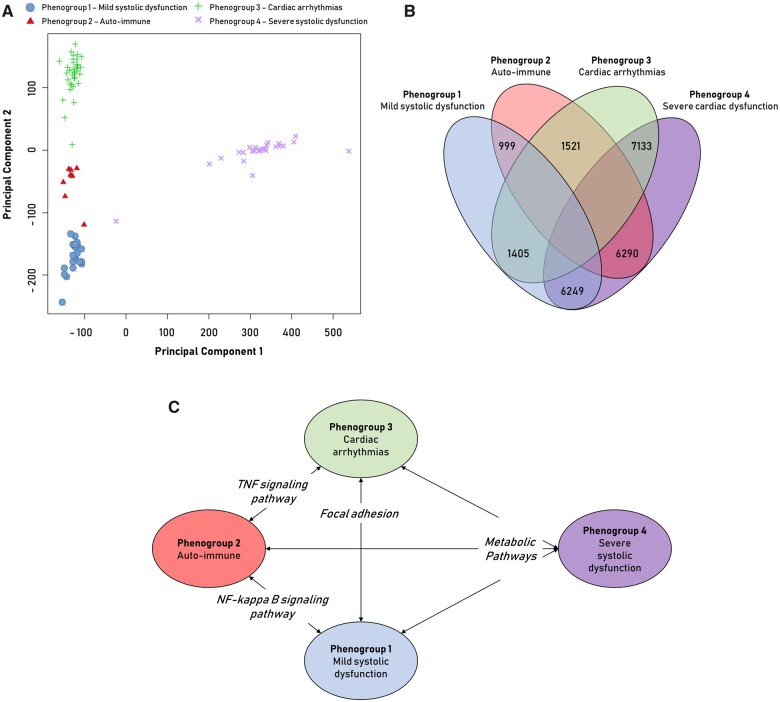
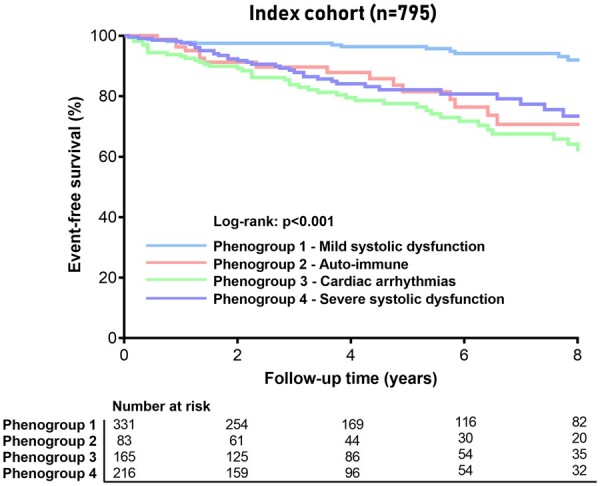
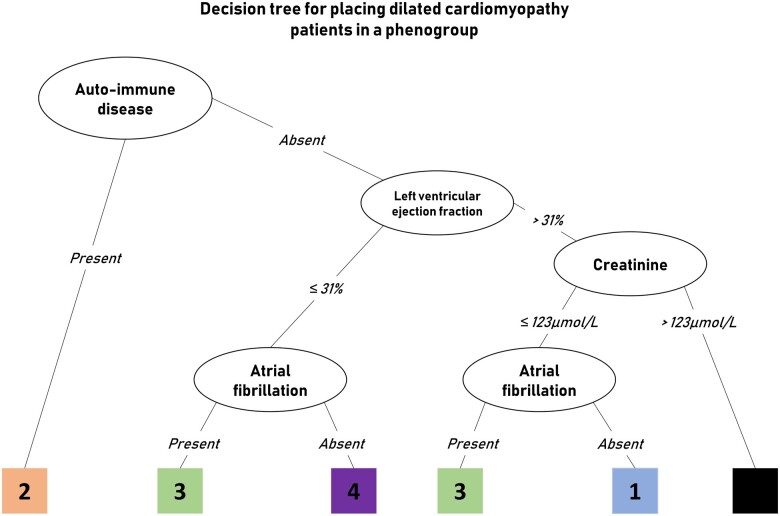
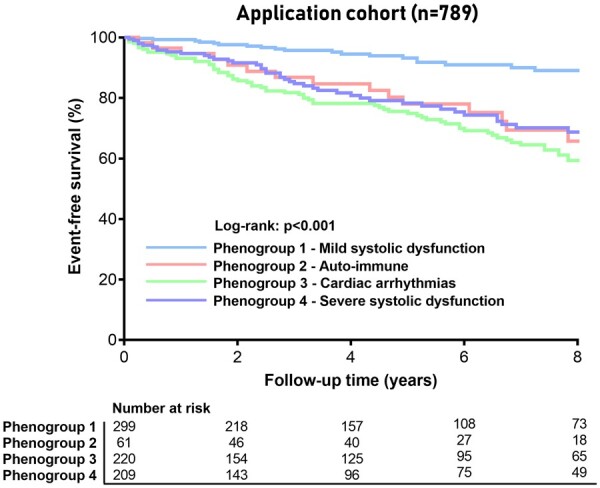
Methods and results: We included 795 consecutive DCM patients from the Maastricht Cardiomyopathy Registry who underwent in-depth phenotyping, comprising extensive clinical data on aetiology and comorbodities, imaging and endomyocardial biopsies. Four mutually exclusive and clinically distinct phenogroups (PG) were identified based upon unsupervised hierarchical clustering of principal components: [PG1] mild systolic dysfunction, [PG2] auto-immune, [PG3] genetic and arrhythmias, and [PG4] severe systolic dysfunction. RNA-sequencing of cardiac samples (n = 91) revealed a distinct underlying molecular profile per PG: pro-inflammatory (PG2, auto-immune), pro-fibrotic (PG3; arrhythmia), and metabolic (PG4, low EF) gene expression. Furthermore, event-free survival differed among the four phenogroups, also when corrected for well-known clinical predictors. Decision tree modelling identified four clinical parameters (auto-immune disease, EF, atrial fibrillation, and kidney function) by which every DCM patient from two independent DCM cohorts could be placed in one of the four phenogroups with corresponding outcome (n = 789; Spain, n = 352 and Italy, n = 437), showing a feasible applicability of the phenogrouping.
Conclusion: The present study identified four different DCM phenogroups associated with significant differences in clinical presentation, underlying molecular profiles and outcome, paving the way for a more personalized treatment approach.
Keywords: Clustering; Dilated cardiomyopathy; Machine learning; Pathophysiology.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Personalized medicine for dilated cardiomyopathy.Eur Heart J. 2021 Jan 7;42(2):175-177. doi: 10.1093/eurheartj/ehaa869. Eur Heart J. 2021. PMID: 33175136 No abstract available.
References
-
- Sinagra G, Elliott PM, Merlo M. Dilated cardiomyopathy: so many cardiomyopathies! Eur Heart J 2019;doi: 10.1093/eurheartj/ehz908. - PubMed
-
- Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck K-H, Hernandez-Madrid A, Nikolaou N, Norekvål TM, Spaulding C, Van Veldhuisen DJ. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J 2015;36:2793–2867. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, Gonzalez-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016;37:2129–2200. - PubMed
-
- Verdonschot JAJ, Hazebroek MR, Derks KWJ, Barandiaran Aizpurua A, Merken JJ, Wang P, Bierau J, van den Wijngaard A, Schalla SM, Abdul Hamid MA, van Bilsen M, van Empel VPM, Knackstedt C, Brunner-La Rocca HP, Brunner HG, Krapels IPC, Heymans SRB. Titin cardiomyopathy leads to altered mitochondrial energetics, increased fibrosis and long-term life-threatening arrhythmias. Eur Heart J 2018;39:864–873. - PubMed
