

Clinical usefulness of tomographic standards for COVID-19 pneumonia diagnosis: Experience from a Brazilian reference center
- PMID: 33157033
- PMCID: PMC7603997
- DOI: 10.1016/j.bjid.2020.10.002
Clinical usefulness of tomographic standards for COVID-19 pneumonia diagnosis: Experience from a Brazilian reference center
Abstract
Background: COVID-19 is a new disease and the most common complication is pneumonia. The Radiological Society of North America (RSNA) proposed an expert consensus for imaging classification for COVID-19 pneumonia.
Objective: To evaluate sensitivity, specificity, accuracy, and reproducibility of chest CT standards in the beginning of the Brazilian COVID-19 outbreak.
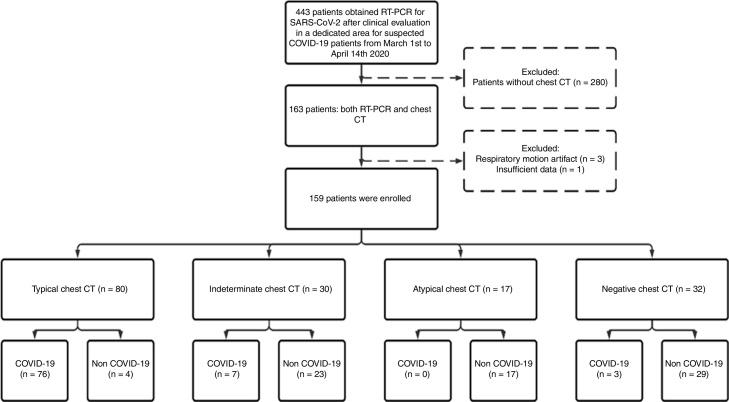
Methods: Cross-sectional study performed from March 1st to April 14th, 2020. Patients with suspected COVID-19 pneumonia submitted to RT-PCR test and chest computed tomography (CT) were included. Two thoracic radiologists blinded for RT-PCR and clinical and laboratory results classified every patient scan according to the RSNA expert consensus. A third thoracic radiologist also evaluated in case of discordance, and consensus was reached among the three radiologists. A typical appearance was considered a positive chest CT for COVID-19 pneumonia. Sensitivity, specificity, positive and negative predictive values were calculated. Cohen's kappa coefficient was used to evaluate intra- and inter-rater agreements.
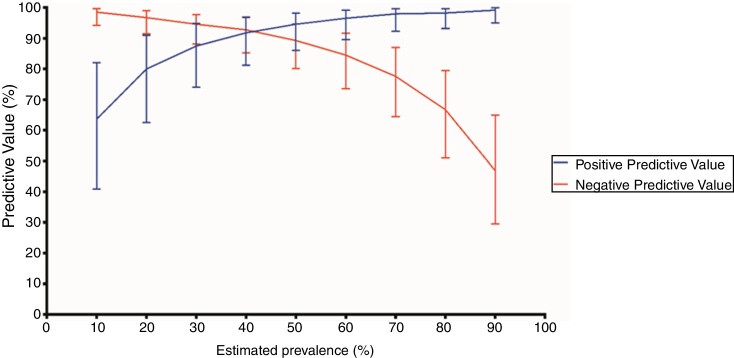
Results: A total of 159 patients were included (mean age 57.9 ± 18.0 years; 88 [55.3%] males): 86 (54.1%) COVID-19 and 73 (45.9%) non-COVID-19 patients. Eighty (50.3%) patients had a positive CT for COVID-19 pneumonia. Sensitivity and specificity of typical appearance were 88.3% (95%CI, 79.9-93.5) and 94.5% (95%CI, 86.7-97.8), respectively. Intra- and inter-rater agreement were assessed (Cohen's kappa = 0.924, P = 0.06; Cohen's kappa=0.772, P = 0.05, respectively).
Conclusion: Chest CT categorical classification of COVID-19 findings is reproducible and demonstrates high level of agreement with clinical and RT-PCR diagnosis of COVID-19. In RT-PCR scarcity scenarios or in equivocal cases, it may be useful for attending physicians in the evaluation of suspected COVID-19 pneumonia patients attended at the emergency unit.
Keywords: CT; Coronavirus disease 2019; Diagnosis.; Viral pneumonia.
Copyright © 2020 Sociedade Brasileira de Infectologia. Published by Elsevier España, S.L.U. All rights reserved.
Figures

Similar articles
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Sep 30;9:CD013639. doi: 10.1002/14651858.CD013639.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. PMID: 32997361 Updated.
-
Chest CT in patients with a moderate or high pretest probability of COVID-19 and negative swab.Radiol Med. 2020 Dec;125(12):1260-1270. doi: 10.1007/s11547-020-01269-w. Epub 2020 Aug 29. Radiol Med. 2020. PMID: 32862406 Free PMC article.
-
Performance of Chest Computed Tomography in Differentiating Coronavirus Disease 2019 From Other Viral Infections Using a Standardized Classification.J Thorac Imaging. 2021 Jan;36(1):31-36. doi: 10.1097/RTI.0000000000000563. J Thorac Imaging. 2021. PMID: 33003105
-
Diagnostic performance between CT and initial real-time RT-PCR for clinically suspected 2019 coronavirus disease (COVID-19) patients outside Wuhan, China.Respir Med. 2020 Jul;168:105980. doi: 10.1016/j.rmed.2020.105980. Epub 2020 Apr 21. Respir Med. 2020. PMID: 32364959 Free PMC article.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Mar 16;3:CD013639. doi: 10.1002/14651858.CD013639.pub4. PMID: 33242342 Updated.
Cited by
-
Omnidirectional 2.5D representation for COVID-19 diagnosis using chest CTs.J Vis Commun Image Represent. 2023 Mar;91:103775. doi: 10.1016/j.jvcir.2023.103775. Epub 2023 Jan 31. J Vis Commun Image Represent. 2023. PMID: 36741546 Free PMC article.
-
Diagnostic performance of the RSNA-proposed classification for COVID-19 pneumonia versus pre-pandemic controls.Braz J Infect Dis. 2022 Jan-Feb;26(1):101665. doi: 10.1016/j.bjid.2021.101665. Epub 2021 Dec 18. Braz J Infect Dis. 2022. PMID: 34958741 Free PMC article.
-
Diagnostic value of chest computed tomography imaging for COVID-19 based on reverse transcription-polymerase chain reaction: a meta-analysis.Infect Dis Poverty. 2021 Oct 21;10(1):126. doi: 10.1186/s40249-021-00910-8. Infect Dis Poverty. 2021. PMID: 34674774 Free PMC article.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2022 May 16;5(5):CD013639. doi: 10.1002/14651858.CD013639.pub5. Cochrane Database Syst Rev. 2022. PMID: 35575286 Free PMC article.
-
Validation of the North America expert consensus statement on reporting CT findings for COVID-19 in individuals with lung cancer.Braz J Med Biol Res. 2023 Jan 9;55:e12376. doi: 10.1590/1414-431X2022e12376. eCollection 2023. Braz J Med Biol Res. 2023. PMID: 36629525 Free PMC article.
References
-
- ACR Recommendations for the use of Chest Radiography and Computed Tomography (CT) for Suspected COVID-19 Infection. https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recom.... Published, 2020. Accessed June 21, 2020.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
