

Management of intussusception in children: A systematic review
- PMID: 33158508
- PMCID: PMC7920908
- DOI: 10.1016/j.jpedsurg.2020.09.055
Management of intussusception in children: A systematic review
Abstract
Objective: The goal of this systematic review by the American Pediatric Surgical Association Outcomes and Evidence-Based Practice Committee was to develop recommendations for the management of ileocolic intussusception in children.
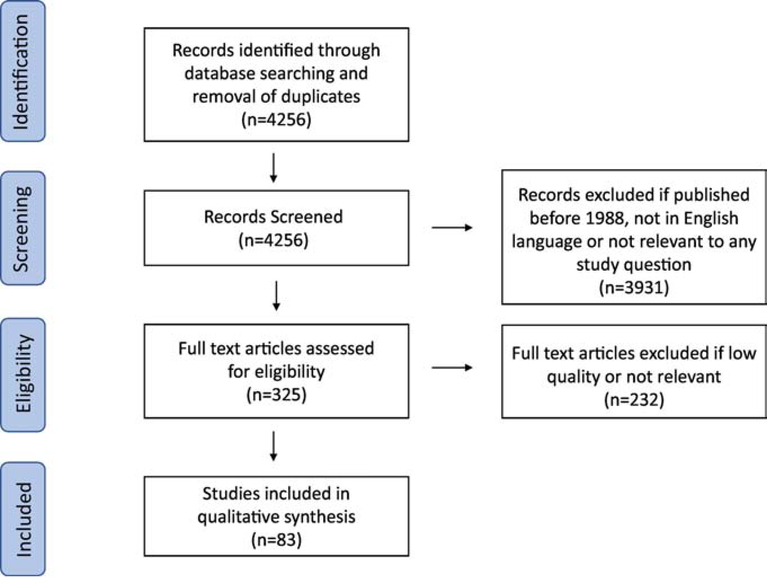
Methods: The ClinicalTrials.gov, Embase, PubMed, and Scopus databases were queried for literature from January 1988 through December 2018. Search terms were designed to address the following topics in intussusception: prophylactic antibiotic use, repeated enema reductions, outpatient management, and use of minimally invasive techniques for children with intussusception. The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines were followed. Consensus recommendations were derived based on the best available evidence.
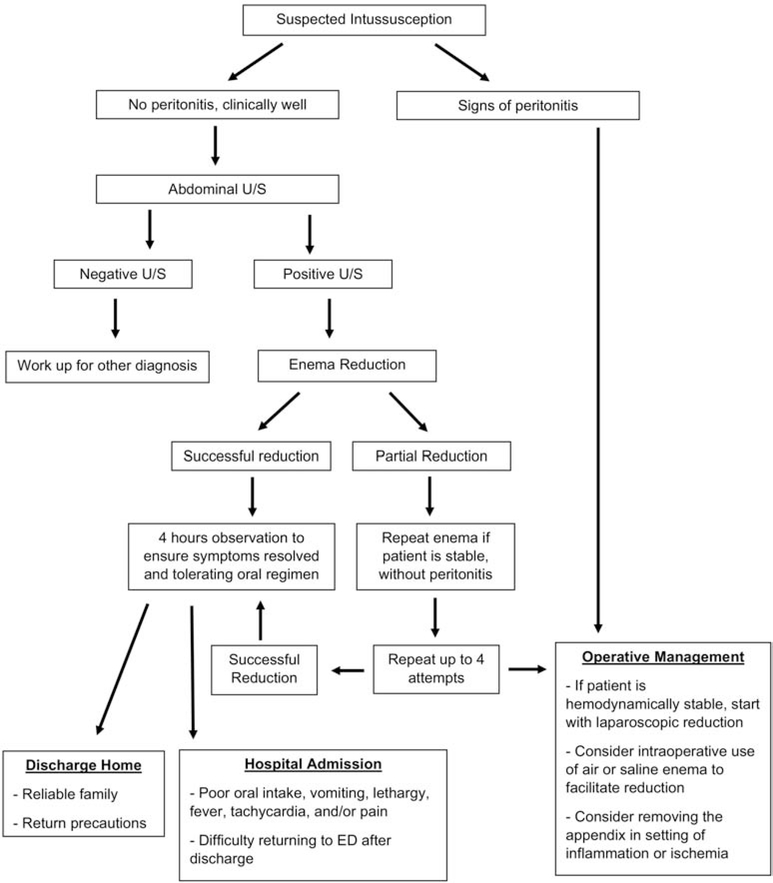
Results: A total of 83 articles were analyzed and included for review. Prophylactic antibiotic use does not decrease complications after radiologic reduction. Repeated enema reductions may be attempted when clinically appropriate. Patients can be safely observed in the emergency department following enema reduction of ileocolic intussusception, avoiding hospital admission. Laparoscopic reduction is often successful.
Conclusions: Regarding intussusception in hemodynamically stable children without critical illness, pre-reduction antibiotics are unnecessary, non-operative outpatient management should be maximized, and minimally invasive techniques may be used to avoid laparotomy.
Level of evidence: Level 3-5 (mainly level 3-4) TYPE OF STUDY: Systematic Review of level 1-4 studies.
Keywords: enema; intussusception; outpatient; surgery.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
