

Perioperative SARS-CoV-2 infections increase mortality, pulmonary complications, and thromboembolic events: A Dutch, multicenter, matched-cohort clinical study
- PMID: 33158548
- PMCID: PMC7513767
- DOI: 10.1016/j.surg.2020.09.022
Perioperative SARS-CoV-2 infections increase mortality, pulmonary complications, and thromboembolic events: A Dutch, multicenter, matched-cohort clinical study
Abstract
Background: A direct comparison of severe acute respiratory syndrome coronavirus 2 positive patients with a severe acute respiratory syndrome coronavirus 2 negative control group undergoing an operative intervention during the current pandemic is lacking, and a reliable estimate of the assumed difference in morbidity and mortality between both patient categories remains unknown.
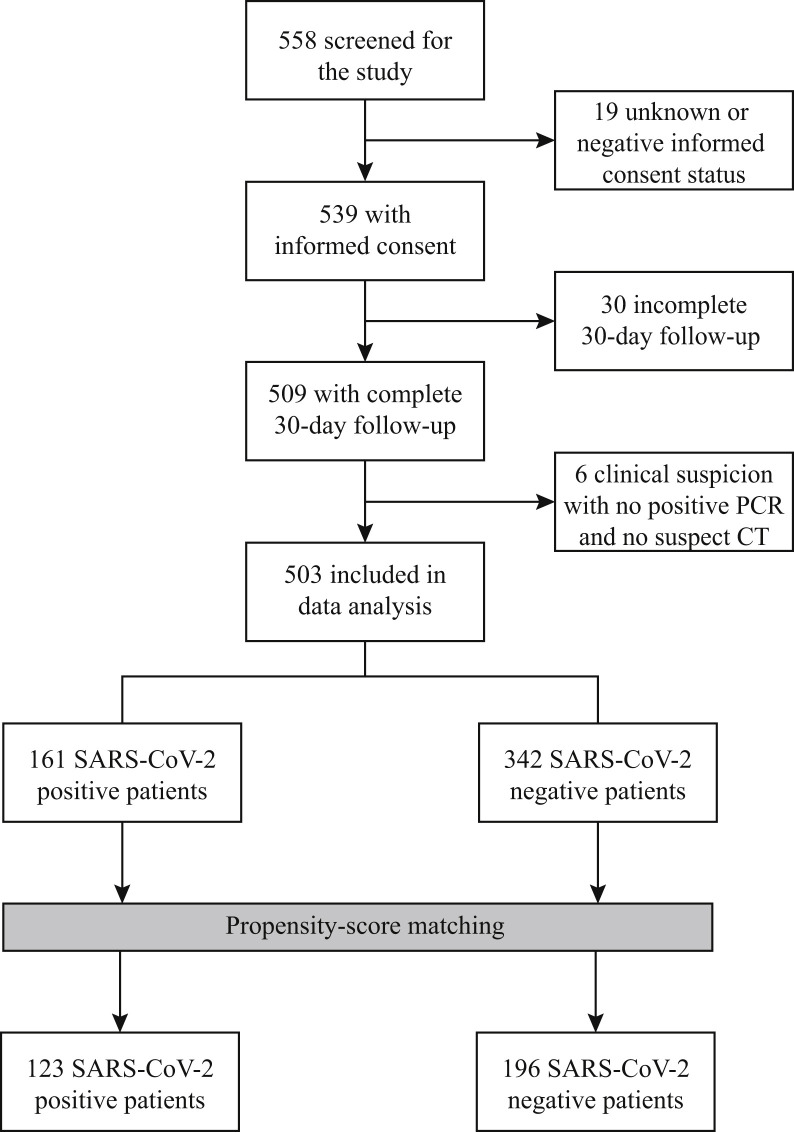
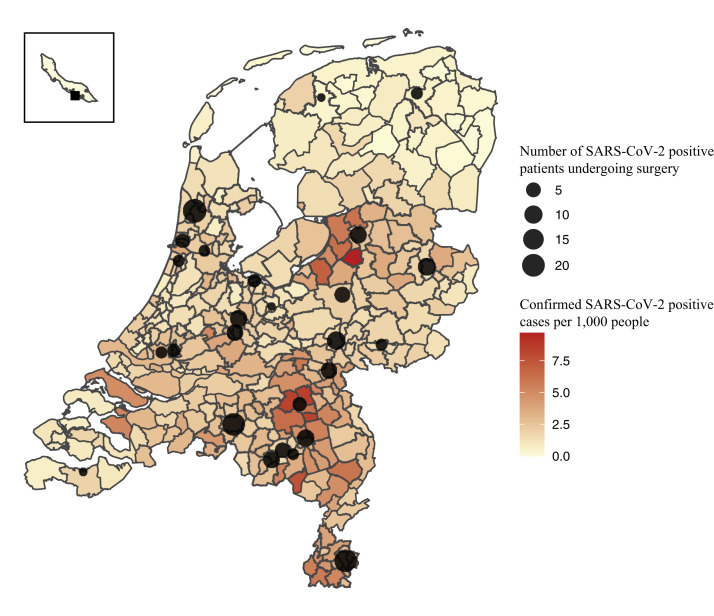
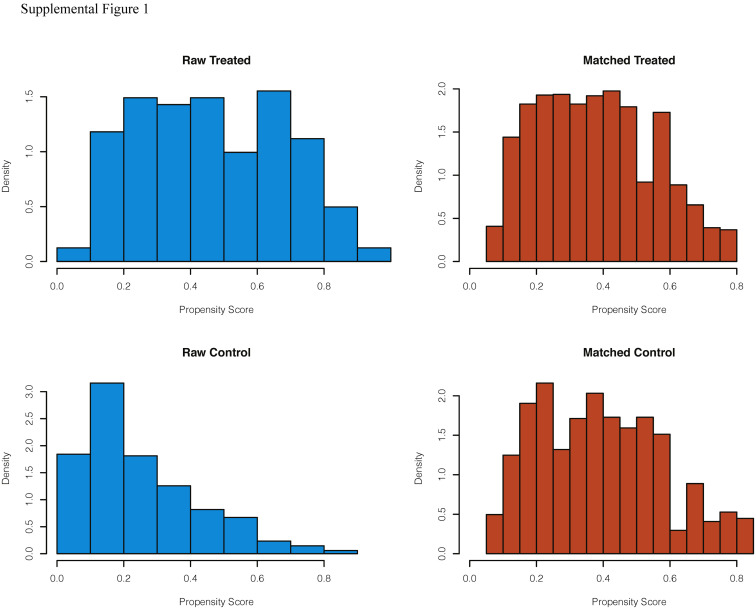
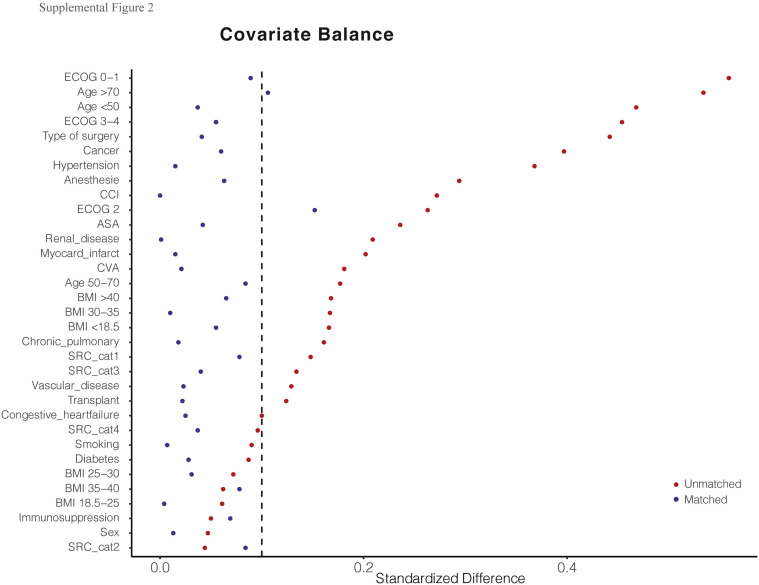
Methods: We included all consecutive patients with a confirmed pre- or postoperative severe acute respiratory syndrome coronavirus 2 positive status (operated in 27 hospitals) and negative control patients (operated in 4 hospitals) undergoing emergency or elective operations. A propensity score-matched comparison of clinical outcomes was performed between severe acute respiratory syndrome coronavirus 2 positive and negative tested patients (control group). Primary outcome was overall 30-day mortality rate between both groups. Main secondary outcomes were overall, pulmonary, and thromboembolic complications.
Results: In total, 161 severe acute respiratory syndrome coronavirus 2 positive and 342 control severe acute respiratory syndrome coronavirus 2 negative patients were included in this study. The 30-day overall postoperative mortality rate was greater in the severe acute respiratory syndrome coronavirus 2 positive cohort compared with the negative control group (16% vs 4% respectively; P = .007). After propensity score matching, the severe acute respiratory syndrome coronavirus 2 positive group consisted of 123 patients (median 70 years of age [interquartile range 59-77] and 55% male) were compared with 196 patients in the matched control group (median 69 years (interquartile range 58-75] and 53% male). The 30-day mortality rate and risk were greater in the severe acute respiratory syndrome coronavirus 2 positive group compared with the matched control group (12% vs 4%; P = .009 and odds ratio 3.4 [95% confidence interval 1.5-8.5]; P = .005, respectively). Overall, pulmonary and thromboembolic complications occurred more often in severe acute respiratory syndrome coronavirus 2 positive patients (P < .01).
Conclusion: Patients diagnosed with perioperative severe acute respiratory syndrome coronavirus 2 have an increased risk of 30-day mortality, pulmonary complications, and thromboembolic events. These findings serve as an evidence-based argument to postpone elective surgery and selected emergency cases.
Copyright © 2020 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Johns Hopkins University of Medicine COVID-19 Map. 2020. https://coronavirus.jhu.edu/map.html
-
- Kiermeier A., Babidge W.J., McCulloch G.A.J., Maddern G.J., Watters D.A., Aitken R.J. National surgical mortality audit may be associated with reduced mortality after emergency admission. ANZ J Surg. 2017;87:830–836. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
