

Comparison of the demographic characteristics and comorbidities of patients with COVID-19 who died in Spanish hospitals based on whether they were or were not admitted to an intensive care unit
- PMID: 33158594
- PMCID: PMC7676372
- DOI: 10.1016/j.medin.2020.09.002
Comparison of the demographic characteristics and comorbidities of patients with COVID-19 who died in Spanish hospitals based on whether they were or were not admitted to an intensive care unit
Abstract
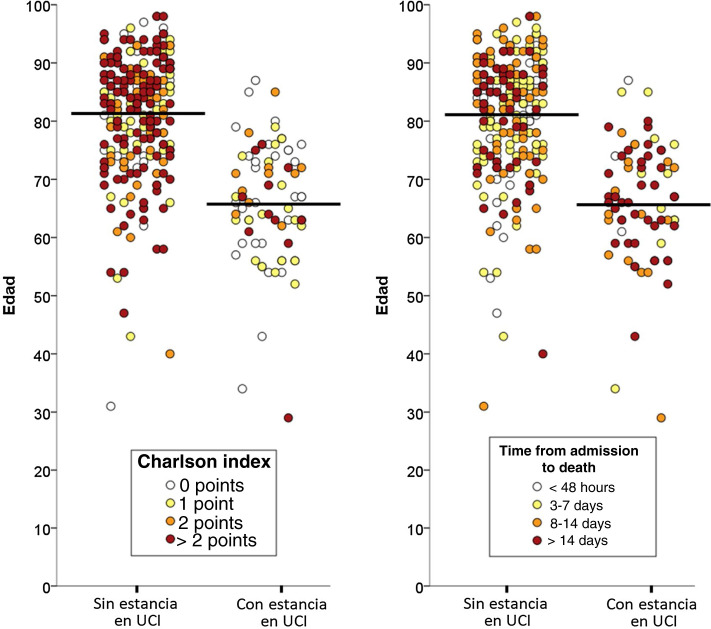
Objective: To describe and compare the demographic characteristics and comorbidities of patients with COVID-19 who died in Spanish hospitals during the 2020 pandemic based on whether they were or were not admitted to an intensive care unit (ICU) prior to death.
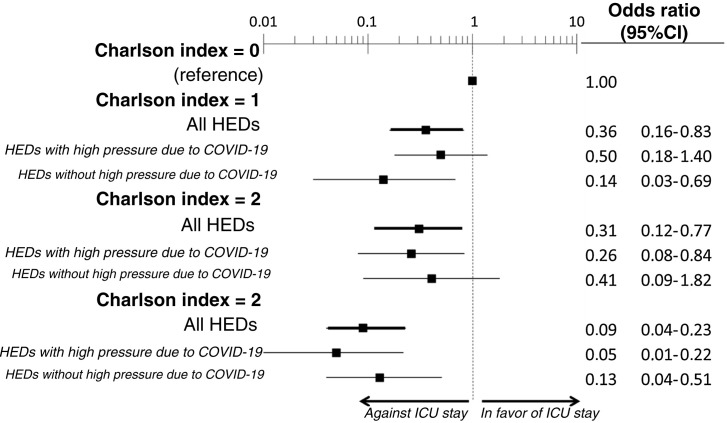
Methods: We performed a secondary analysis of COVID-19 patients who died during hospitalization included by 62 Spanish emergency departments in the SIESTA cohort. We collected the demographic characteristics and comorbidities, determined both individually and estimated globally by the Charlson index (ChI). Independent factors related to ICU admission were identified and different analyses of sensitivity were performed to contrast the consistency of the findings of the principal analysis.
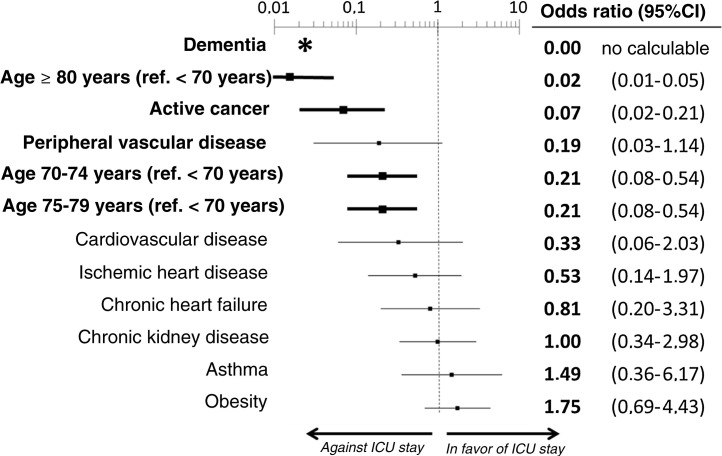
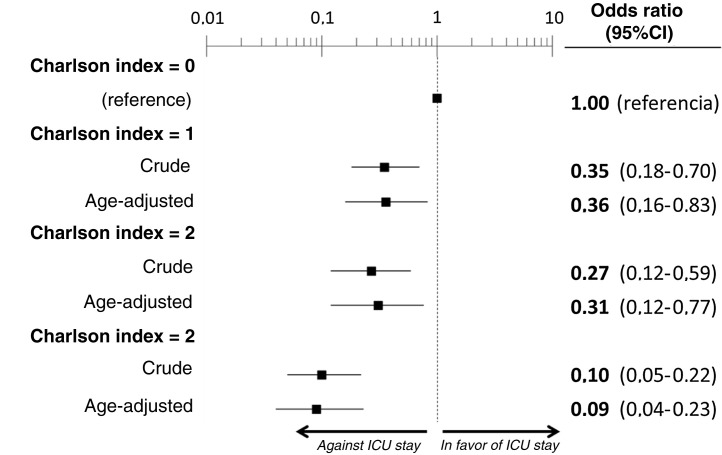
Results: We included the 338 patients from the SIESTA cohort that died during hospitalization. Of these, 77 (22.8%) were admitted to an ICU before dying. After multivariate adjustment, 3 out of the 20 basal characteristics analyzed in the present study were independently associated with ICU admission: dementia (no patients with dementia who died were admitted to the ICU: OR = 0, 95%CI = not calculable), active cancer (OR = 0.07; 95%CI = 0.02-0.21) and age (< 70 years: OR = 1, reference; 70-74 years: OR = 0.21; 95%CI = 0.08-0.54; 75-79 years: OR = 0.21; 95%CI = 0.08-0.54; ≥ 80 years: OR = 0.02; 95%CI = 0.01-0.05). The probability of ICU admission significantly increased in parallel to the ChI, even after adjustment for age (ChI 0 points: OR = 0, reference; ChI 1 point: OR = 0.36; 95%CI = 0.16-0.83; ChI 2 points: OR = 0.36; 95%CI = 0.16-0.83; ChI >2 points: OR = 0.09; 95%CI = 0.04-0.23). The sensitivity analyses showed no gross differences compared to the principal analysis.
Conclusions: The profile of COVID-19 patients who died without ICU admission is similar to that observed in the usual medical practice before the pandemic. The basal characteristics limiting their admission were age and global burden due to comorbidity, especially dementia and active cancer.
Objetivo: Describir las características demográficas y de comorbilidad de los pacientes con COVID-19 fallecidos en hospitales españoles durante el brote pandémico de 2020 y compararlas según si ingresaron o no en una Unidad de Cuidados Intensivos (UCI) antes del fallecimiento.
Métodos: Análisis secundario de los pacientes de la cohorte SIESTA (formada por pacientes COVID de 62 hospitales españoles) fallecidos durante la hospitalización. Se recogieron sus características demográficas y comorbilidades, individuales y globalmente, estimadas mediante el índice de comorbilidad de Charlson (ICC). Se identificaron los factores independientes relacionados con ingreso en UCI, y se realizaron diversos análisis de sensibilidad para contrastar la consistencia de los hallazgos del análisis principal.
Resultados: Se incluyeron los 338 pacientes de la cohorte SIESTA fallecidos; de ellos, 77 (22,8%) accedieron a una UCI previamente al fallecimiento. En el análisis multivariable, tres de las 20 características basales analizadas se asociaron independientemente con ingreso en UCI de los pacientes fallecidos: demencia (no hubo pacientes fallecidos con demencia que ingresasen en UCI; OR = 0, IC 95% = no calculable), cáncer activo (OR = 0,07, IC 95% = 0,02-0,21) y edad (<70 años: OR = 1, referencia; 70-74 años: OR = 0,21, IC 95% = 0,08-0,54; 75-79 años: OR = 0,21, IC 95% = 0,08-0,54; ≥ 80 años: OR = 0,02, IC 95% = 0,01-0,05). La probabilidad de ingreso en UCI de los pacientes que fallecieron disminuyó significativamente al aumentar el ICC, incluso tras ajustarla por edad (ICC 0 puntos: OR = 1, referencia; ICC 1 punto: OR = 0,36, IC 95% = 0,16-0,83; ICC 2 puntos: OR = 0,36, IC 95% = 0,16-0,83; ICC > 2 puntos: OR = 0,09, IC 95% = 0,04-0,23). Los análisis de sensibilidad no mostraron diferencias destacables respecto al análisis principal.
Conclusiones: El perfil de los pacientes COVID fallecidos sin ingresar en UCI se ajustó a lo observado en la práctica médica habitual antes de la pandemia, y las características basales que limitaron su ingreso fueron la edad y la carga de comorbilidad global, especialmente la demencia y el cáncer activo.
Keywords: COVID-19; Características clínicas; Clinical characteristics; Comorbidities; Comorbilidades; Emergency departments; SARS-CoV-2; Servicios de urgencias.
Copyright © 2020 Elsevier España, S.L.U. y SEMICYUC. All rights reserved.
Figures
Similar articles
-
Analysis of clinical characteristics and outcomes in patients with COVID-19 based on a series of 1000 patients treated in Spanish emergency departments.Emergencias. 2020 Ago;32(4):233-241. Emergencias. 2020. PMID: 32692000 English, Spanish.
-
Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy.JAMA. 2020 Apr 28;323(16):1574-1581. doi: 10.1001/jama.2020.5394. JAMA. 2020. PMID: 32250385 Free PMC article.
-
Characteristics and outcomes of patients hospitalized for COVID-19 in France: The Critical COVID-19 France (CCF) study.Arch Cardiovasc Dis. 2021 May;114(5):352-363. doi: 10.1016/j.acvd.2021.01.003. Epub 2021 Mar 2. Arch Cardiovasc Dis. 2021. PMID: 34154953 Free PMC article.
-
[Evolution of patients infected with SARS-CoV-2 according to previous metabolic status].Nutr Hosp. 2021 Oct 13;38(5):1068-1074. doi: 10.20960/nh.03469. Nutr Hosp. 2021. PMID: 34176273 Spanish.
-
Global Impact of Coronavirus Disease 2019 Infection Requiring Admission to the ICU: A Systematic Review and Meta-analysis.Chest. 2021 Feb;159(2):524-536. doi: 10.1016/j.chest.2020.10.014. Epub 2020 Oct 15. Chest. 2021. PMID: 33069725 Free PMC article.
Cited by
-
Case Report: Massive Spontaneous Pneumothorax-A Rare Form of Presentation for Severe COVID-19 Pneumonia.Medicina (Kaunas). 2021 Jan 20;57(2):82. doi: 10.3390/medicina57020082. Medicina (Kaunas). 2021. PMID: 33498180 Free PMC article.
-
Spatio-temporal multidisciplinary analysis of socio-environmental conditions to explore the COVID-19 early evolution in urban sites in South America.Heliyon. 2023 May 6;9(5):e16056. doi: 10.1016/j.heliyon.2023.e16056. eCollection 2023 May. Heliyon. 2023. PMID: 37200576 Free PMC article.
-
Spontaneous Pneumothorax as a Late Complication of Mild COVID-19 Infection: A Case Report.Cureus. 2022 Mar 18;14(3):e23294. doi: 10.7759/cureus.23294. eCollection 2022 Mar. Cureus. 2022. PMID: 35449691 Free PMC article.
-
Incidence, Clinical Characteristics, Risk Factors and Outcomes of Acute Coronary Syndrome in Patients With COVID-19: Results of the UMC-19-S1010.J Emerg Med. 2022 Apr;62(4):443-454. doi: 10.1016/j.jemermed.2021.10.046. Epub 2021 Nov 3. J Emerg Med. 2022. PMID: 35065863 Free PMC article.
-
COVID-19 Mortality Rate and Its Incidence in Latin America: Dependence on Demographic and Economic Variables.Int J Environ Res Public Health. 2021 Jun 27;18(13):6900. doi: 10.3390/ijerph18136900. Int J Environ Res Public Health. 2021. PMID: 34199070 Free PMC article.
References
-
- Martín-Sánchez F.J., González del Castillo J., Valls Carbó A., López Picado A., Martínez-Valero C., Miranda J.D., et al. Categorías diagnósticas y resultados a corto plazo en los pacientes con sospecha de COVID-19 atendidos en un servicio de urgencias. Emergencias. 2020;32:242–252. - PubMed
-
- Rodríguez A., Moreno G., Gómez J., Carbonell R., Picó-Plana E., Benavent Bofill C., et al. Infección grave por coronavirus SARS-CoV-2: experiencia en un hospital de tercer nivel con pacientes afectados por COVID-19 durante la pandemia 2020. Med Intensiva. 2020 doi: 10.1016/j.medin.2020.05.018. in press. - DOI - PMC - PubMed
-
- González del Castillo J., Cánora Lebrato J., Zapatero Gaviria A., Barba Martín R., Prados Roa F., Marco Martínez J. Epidemia por COVID-19 en Madrid: crónica de un reto. Emergencias. 2020;32:191–193. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
