

Ticagrelor Added to Aspirin in Acute Ischemic Stroke or Transient Ischemic Attack in Prevention of Disabling Stroke: A Randomized Clinical Trial
- PMID: 33159526
- PMCID: PMC7648910
- DOI: 10.1001/jamaneurol.2020.4396
Ticagrelor Added to Aspirin in Acute Ischemic Stroke or Transient Ischemic Attack in Prevention of Disabling Stroke: A Randomized Clinical Trial
Erratum in
-
Error in Figure.JAMA Neurol. 2021 Feb 1;78(2):253. doi: 10.1001/jamaneurol.2020.4906. JAMA Neurol. 2021. PMID: 33346782 Free PMC article. No abstract available.
Abstract
Importance: Reduction of subsequent disabling stroke is the main goal of preventive treatment in the acute setting after transient ischemic attack (TIA) or minor ischemic stroke.
Objective: To evaluate the superiority of ticagrelor added to aspirin in preventing disabling stroke and to understand the factors associated with recurrent disabling stroke.
Design, setting, and participants: The Acute Stroke or Transient Ischemic Attack Treated With Ticagrelor and Aspirin for Prevention of Stroke and Death (THALES) was a randomized clinical trial conducted between January 22, 2018, and December 13, 2019, with a 30-day follow-up, at 414 hospitals in 28 countries. The trial included 11 016 patients with a noncardioembolic, nonsevere ischemic stroke or high-risk TIA, including 10 803 with modified Rankin Scale score (mRS) recorded at 30 days.
Interventions: Ticagrelor (180-mg loading dose on day 1 followed by 90 mg twice daily for days 2-30) or placebo within 24 hours of symptom onset. All patients received aspirin, 300 to 325 mg on day 1 followed by 75 to 100 mg daily for days 2 to 30.
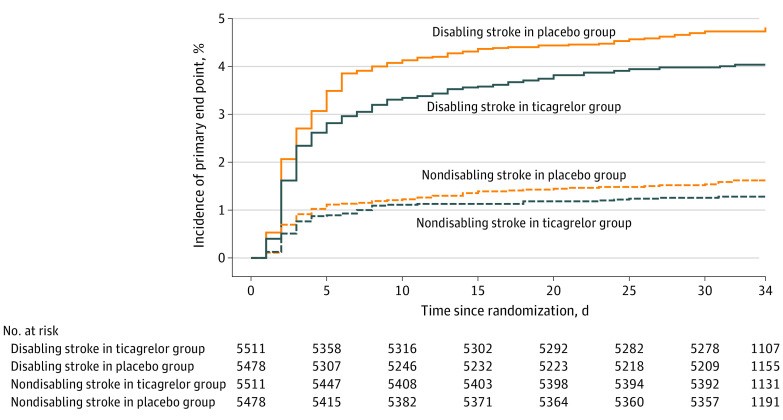
Main outcomes and measures: Time to the occurrence of disabling stroke (progression of index event or new stroke) or death within 30 days, as measured by mRS at day 30. Disabling stroke was defined by mRS greater than 1.
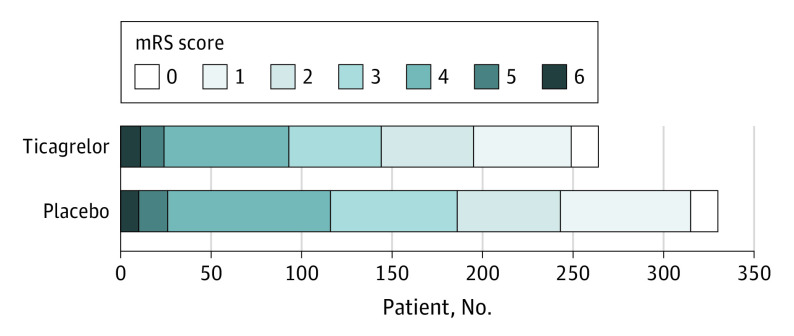
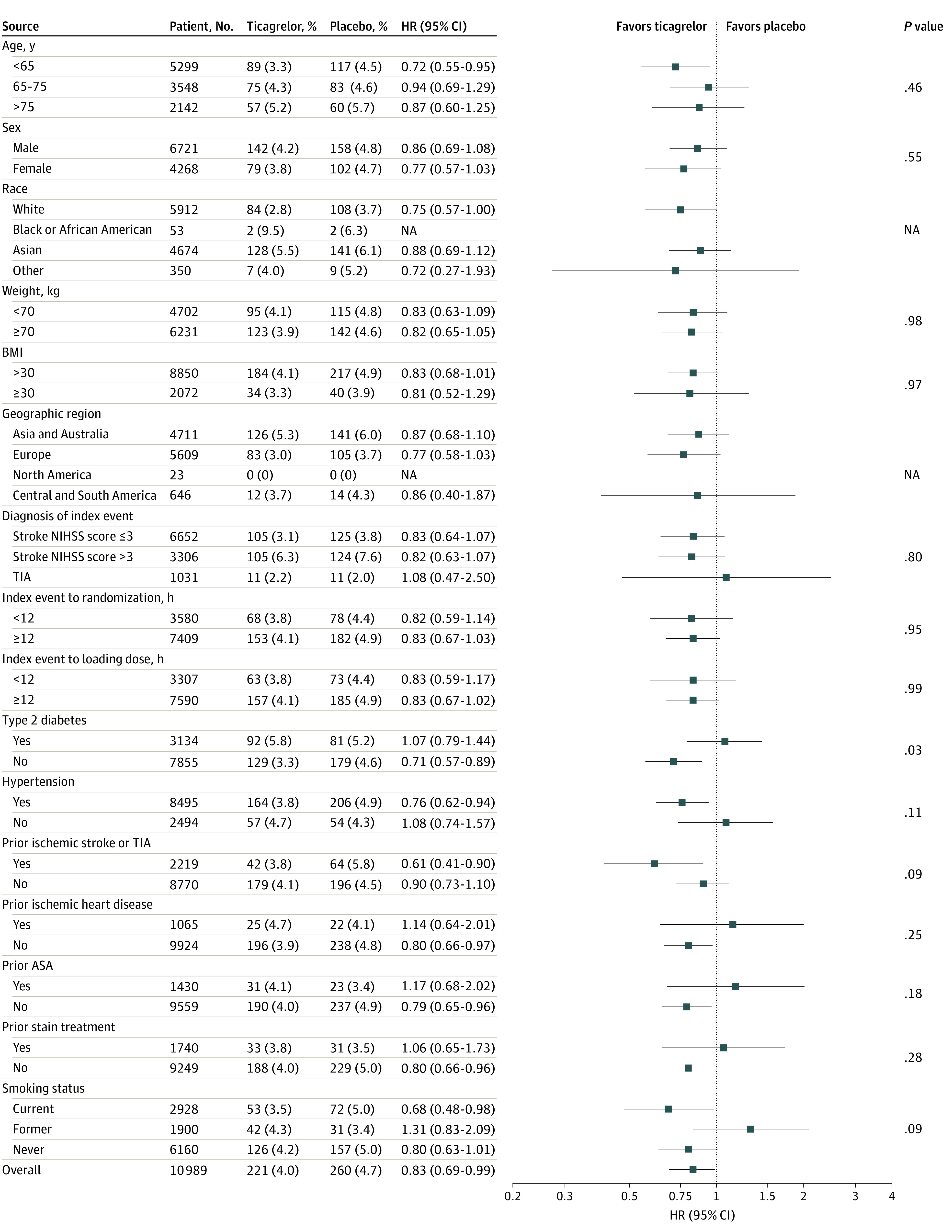
Results: Among participants with 30-day mRS greater than 1, mean age was 68.1 years, 1098 were female (42.6%), and 2670 had an ischemic stroke (95.8%) as a qualifying event. Among 11 016 patients, a primary end point with mRS greater than 1 at 30 days occurred in 221 of 5511 patients (4.0%) randomized to ticagrelor and in 260 of 5478 patients (4.7%) randomized to placebo (hazard ratio [HR], 0.83; 95% CI, 0.69-0.99, P = .04). A primary end point with mRS 0 or 1 at 30 days occurred in 70 of 5511 patients (1.3%) and 87 of 5478 patients (1.6%) (HR, 0.79; 95% CI, 0.57-1.08; P = .14). The ordinal analysis of mRS in patients with recurrent stroke showed a shift of the disability burden following a recurrent ischemic stroke in favor of ticagrelor (odds ratio, 0.77; 95% CI, 0.65-0.91; P = .002). Factors associated with disability were baseline National Institutes of Health Stroke Scale score 4 to 5, ipsilateral stenosis of at least 30%, Asian race/ethnicity, older age, and higher systolic blood pressure, while treatment with ticagrelor was associated with less disability.
Conclusions and relevance: In patients with TIA and minor ischemic stroke, ticagrelor added to aspirin was superior to aspirin alone in preventing disabling stroke or death at 30 days and reduced the total burden of disability owing to ischemic stroke recurrence.
Trial registration: ClinicalTrials.gov Identifier: NCT03354429.
Conflict of interest statement
Figures
References
-
- Rothwell PM, Algra A, Chen Z, Diener HC, Norrving B, Mehta Z. Effects of aspirin on risk and severity of early recurrent stroke after transient ischaemic attack and ischaemic stroke: time-course analysis of randomised trials. Lancet. 2016;388(10042):365-375. doi: 10.1016/S0140-6736(16)30468-8 - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
